Am I in Perimenopause? A Checklist by Age (40–55)
Am I in perimenopause? Use our age-specific perimenopause checklist to compare your symptoms at 40, 45, or 50. Understand what's normal, what to track, and when to see your doctor.
Perimenopause Compasss
2/12/202615 min read
You've been Googling at midnight. Maybe it started with "why am I so tired at 43" or "sudden anxiety at 45" or "period every 24 days." And somewhere — between the WebMD rabbit hole and a Reddit thread from three years ago — the word popped up.
Perimenopause.
And now you're wondering: is that what this is?
You're not alone in asking. And you're not alone in struggling to get a clear answer. "Am I in perimenopause?" is one of the most common — and most frustrating — health questions women in their 40s face. Because there's no single definitive test. Because symptoms are subtle and variable. And because many healthcare providers still don't recognize the early signs.
This article gives you what most resources don't: a practical, age-specific checklist you can use right now to evaluate your symptoms — plus the science, the real-life context, and the clear next steps to help you move from wondering to knowing.
Why So Many Women Wonder — And Why Answers Are Hard to Find
The Problem with "Am I in Perimenopause?"
It seems like it should be a straightforward question. It's not.
Here's why:
There's no single test. Unlike pregnancy or diabetes, there's no one blood test that reliably confirms perimenopause (more on this below).
Symptoms overlap with everything else. Fatigue, anxiety, sleep disruption, brain fog — these could be perimenopause, thyroid issues, stress, depression, or just "life."
It starts gradually. Perimenopause doesn't arrive with a clear starting signal. It creeps in — a slightly shorter cycle here, a new bout of insomnia there — making it easy to explain away each symptom individually.
The timeline varies enormously. Some women start at 38. Others at 48. The average is mid-40s, but "average" doesn't help when you're trying to figure out your own body.
The result: millions of women spend months or years in a diagnostic grey zone — experiencing real hormonal changes but unable to confirm them.
Why Your Doctor Might Not Have the Answer Either
This isn't a criticism of individual doctors. It's a systemic problem.
Research published in Menopause journal has shown that many physicians receive minimal formal training in menopause medicine. A UK survey found that medical schools dedicate an average of just a few hours to menopause education across the entire curriculum.
That means when you walk into an appointment and say "I think I might be perimenopausal," your provider may:
Order a blood test that comes back "normal" and reassure you nothing is wrong
Attribute your symptoms to stress, aging, or depression
Not be familiar with the nuanced, fluctuating nature of early perimenopause
This doesn't mean you shouldn't see your doctor — you absolutely should. But it means you may need to advocate for yourself and come prepared with clear information about your symptoms.
That's exactly what this checklist is designed to help you do.
What Perimenopause Actually Is (And What It Isn't)
Perimenopause vs. Menopause vs. Premenopause — Cleared Up
These terms get mixed up constantly. Let's set the record straight:
Key insight: What most people casually call "menopause" — the years of symptoms — is actually perimenopause. Menopause itself is just one day. The transition is the journey.
The STRAW+10 Stages — Where You Might Be Right Now
The Stages of Reproductive Aging Workshop (STRAW+10) is the internationally recognized system for classifying where a woman is in her reproductive timeline. It divides the transition into specific stages:
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References
Get the Perimenopause Nutrition Protocol ($29 + bonus)
Get the Perimenopause Nutrition Protocol ($29 + bonus)


Most women reading this article are likely somewhere in the early to late perimenopause range — and the checklists below are designed to help you identify where.
How Perimenopause Shows Up Differently at Every Age
Why Symptoms at 41 Look Different from Symptoms at 49
Perimenopause isn't one experience — it's a spectrum that evolves over years. The symptoms you notice at 41 are often very different from what a woman experiences at 49 — because the underlying hormonal shifts are different at each stage.
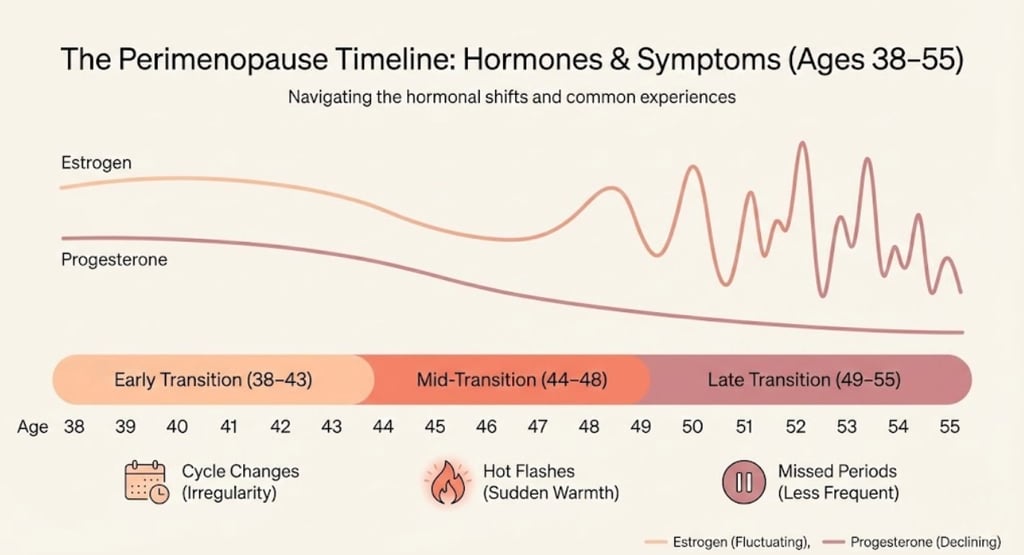
In your early 40s: Progesterone tends to decline first (because ovulation becomes less consistent). Estrogen may still be normal — even higher than usual at times. This creates relative estrogen dominance: worsening PMS, heavier periods, breast tenderness, irritability, and sleep disruption.
In your mid-40s: Estrogen begins its characteristic fluctuations — spiking unpredictably, then crashing. This is when vasomotor symptoms (hot flashes, night sweats) often emerge, and when anxiety, brain fog, and fatigue can intensify.
In your late 40s to early 50s: Estrogen fluctuations widen. Periods become more visibly irregular — longer gaps, skipped months, unexpected bleeding. Symptoms may peak in intensity during the 1–2 years before the final period.
Understanding this progression matters because it changes what you should look for at each age.
The Hormonal Timeline Most Women Are Never Taught
Here's a simplified version of what's happening hormonally — the timeline nobody gave you in health class:
Age 35–40: Fertility begins declining. Subtle hormonal shifts may begin but are rarely symptomatic.
Age 40–44: Progesterone drops as ovulation becomes irregular. Early symptoms may emerge — often dismissed as stress.
Age 44–48: Estrogen fluctuations intensify. The "classic" perimenopause experience takes shape. Cycles change more noticeably.
Age 48–52: Hormonal activity declines more consistently. Periods may stop for months, then return. The approach to menopause.
Age 51 (average): Final menstrual period. But this can range from 45 to 58 normally.
Your timeline is yours. Genetics (when your mother went through menopause), lifestyle, health conditions, and even ethnicity all influence timing and symptom severity.
Your Perimenopause Checklist — Ages 38–43 (Early Transition)
What's likely happening hormonally:
Progesterone is declining as ovulation becomes less consistent. Estrogen may still be stable or even periodically elevated. FSH may be starting to rise, but blood tests at this stage are highly unreliable.
Use this checklist if you're between 38 and 43 and wondering whether what you're feeling might be the beginning of perimenopause.
Check every statement that applies to you over the past 3–6 months:
Cycle Changes to Watch For
☐ My cycles have become shorter (25 days or less instead of my usual 28–30)
☐ My periods are heavier than they used to be — more clotting, more flooding
☐ OR my periods are becoming lighter or shorter than usual
☐ My PMS feels worse — more intense, lasting longer, or different from before
☐ I've noticed breast tenderness that's new or more pronounced
☐ I occasionally have spotting between periods
Mood and Energy Shifts
☐ I've developed anxiety or a sense of dread that feels new and unexplained
☐ I feel more irritable or emotionally reactive — small things trigger big responses
☐ My energy has dropped in a way that rest doesn't fix
☐ I have moments of brain fog — forgetting words, losing focus, feeling mentally sluggish
☐ I feel emotionally fragile — crying more easily or feeling overwhelmed by things I used to handle fine
Physical Signs You Might Dismiss
☐ My sleep has changed — waking at 3–4 a.m., lighter sleep, or trouble falling asleep
☐ I've noticed joint stiffness or new aches — especially in the morning
☐ My libido has shifted — less spontaneous desire or a change in arousal
☐ I've experienced occasional heart palpitations that come and go
☐ I have a gut feeling that something in my body has changed — even if I can't pinpoint it exactly
☐ My hair, skin, or body composition feels subtly different
✅ Your Early Transition Checklist — How to Read Your Results
Your Perimenopause Checklist — Ages 44–48 (Mid-Transition)
What's likely happening hormonally:
Estrogen is fluctuating more dramatically — spiking and crashing unpredictably. Progesterone continues to decline. Ovulation is becoming increasingly inconsistent. FSH is rising. This is typically the most symptomatic phase of perimenopause.
Use this checklist if you're between 44 and 48 and experiencing changes that feel like more than "just stress."
Check every statement that applies over the past 3–6 months:
Cycle and Vasomotor Symptoms
☐ My cycle length has become unpredictable — varying by more than 7 days from month to month
☐ I've had one or more skipped periods (a gap of 45+ days)
☐ My periods alternate between very heavy and very light
☐ I've experienced hot flashes — sudden waves of heat, often in the chest and face
☐ I've had night sweats — waking up damp or having to change clothes/sheets
☐ I've noticed flushing or sudden warmth during the day, even briefly
Mood, Cognition, and Sleep
☐ My anxiety has intensified — including physical symptoms like chest tightness or racing heart
☐ I experience mood swings that feel disproportionate or hard to control
☐ Brain fog is affecting my daily functioning — memory lapses, difficulty concentrating
☐ Insomnia is now a regular issue — difficulty falling asleep, staying asleep, or both
☐ I feel exhausted even after a full night's sleep
☐ I've had episodes of rage or irritability that feel out of character
☐ I've felt low mood or depressive symptoms that are new or different from past experiences
Physical and Systemic Changes
☐ I've noticed weight redistribution — especially around the abdomen — even without major diet changes
☐ Joint pain or stiffness has become more persistent
☐ I experience headaches or migraines that are new or linked to my cycle
☐ My vaginal dryness or discomfort has increased
☐ I notice urinary changes — urgency, frequency, or mild incontinence
☐ My skin feels drier or has changed in texture
☐ Heart palpitations happen more frequently
☐ I've experienced digestive changes — bloating, altered bowel patterns
✅ Your Mid-Transition Checklist — How to Read Your Results
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
⚠️ Important note: If you've had no period for 12 consecutive months, you've reached menopause — the transition is technically complete. If heavy bleeding returns after a gap of 12+ months, see your doctor promptly to rule out other causes.
What Women Actually Experience — The Real Story Behind the Checklist
Checklists are useful. But they don't capture how it feels to live inside this question.
"I Checked Every Box and Still Doubted Myself"
"I went through a checklist like this at 44. I checked 12 out of 15 items. And I still thought — maybe it's just stress. Maybe I need more sleep. Maybe I need to try harder. It took me another year to actually say the word 'perimenopause' to my doctor. And when she confirmed it, I didn't feel alarmed. I felt relieved. I finally had a name for what had been happening."
"My Symptoms Didn't Match the Textbook"
"I expected hot flashes. What I got was rage. Uncontrollable, volcanic, completely-unlike-me rage. I cried in the car after snapping at my kid over nothing. I thought I needed anger management. Turns out, I needed someone to explain that estrogen fluctuations can profoundly affect emotional regulation. No textbook listed 'screaming at your partner about the dishwasher' as a perimenopause symptom — but it should."
"I Wish I'd Known at 42 What I Know Now at 48"
"I spent six years thinking something was wrong with me. That I was weak, broken, falling apart. If someone had sat me down at 42 and said — 'What you're experiencing is a normal hormonal transition, here's what to watch for, and here are your options' — it would have changed everything. Not the symptoms themselves, maybe. But the shame. The isolation. The years of not understanding my own body."
These stories matter because they reflect what research confirms: the psychological burden of not knowing can be as significant as the symptoms themselves. Recognition — even without a formal blood test — is therapeutic.
What Science Says — Can Perimenopause Be Confirmed?
Why Blood Tests Are Unreliable in Perimenopause
This is one of the most common sources of confusion — so let's be clear about it.
The standard blood test for menopause is FSH (Follicle-Stimulating Hormone). In postmenopause, FSH is consistently elevated. It's a reliable marker after the transition is complete.
But in perimenopause — especially early perimenopause — FSH is wildly variable. It can be elevated one week and normal the next. A single measurement is like checking the weather at one moment and trying to predict the whole season.
Other hormonal markers:
Estradiol (estrogen): Fluctuates dramatically during perimenopause — often higher than premenopausal levels at times, then crashing. A normal result doesn't mean you're not perimenopausal.
Progesterone: Declines as ovulation becomes inconsistent, but isn't routinely tested.
AMH (Anti-Müllerian Hormone): Reflects ovarian reserve and declines with age. It can support the picture but isn't a diagnostic test for perimenopause.
The bottom line: A doctor who says "your bloods are normal, so you're not perimenopausal" may be relying on a tool that isn't designed for this purpose.
How Doctors Actually Diagnose the Transition
According to current clinical guidelines — including those from NICE (UK), NAMS (US), and the STRAW+10 criteria — perimenopause is primarily a clinical diagnosis based on:
Age (typically 40+)
Symptom pattern (multiple symptoms consistent with hormonal change)
Menstrual cycle changes (documented shifts in cycle length, flow, or regularity)
Exclusion of other causes (thyroid dysfunction, anemia, depression, etc.)
In women over 45, UK NICE guidelines explicitly state that blood tests are not required to diagnose perimenopause — symptoms and history are sufficient.
In women under 45, testing may be more appropriate to rule out premature ovarian insufficiency (POI) or other conditions.
This is exactly why your symptom checklist and tracking data are so valuable. They provide the clinical picture that a single blood draw cannot.
What Is Established vs. What Is Still Being Studied
Scientifically established:
Perimenopause typically begins 4–8 years before menopause
Hormonal fluctuations (not just decline) drive most symptoms
Sleep, mood, cognition, and vasomotor function are directly affected
Clinical diagnosis based on symptoms is the standard approach
Blood tests are unreliable during the transition
Probable (growing evidence):
Mood and sleep symptoms may precede vasomotor symptoms as the earliest indicators
Individual genetics significantly influence timing and severity
Gut microbiome health affects estrogen metabolism and symptom intensity
Earlier recognition and intervention may improve long-term outcomes
Still debated or under-researched:
Optimal biomarkers for early perimenopause detection
Whether AI-based symptom tracking could improve diagnostic accuracy
The long-term cognitive effects of perimenopausal hormonal changes
Personalized treatment timing based on STRAW staging
This article is for educational purposes and does not replace medical advice. These checklists are self-assessment tools — not diagnostic instruments. If your symptoms are concerning or affecting your quality of life, consult a healthcare provider.
How to Use Your Checklist Results
If You Checked 0–3 Boxes
You may not be in perimenopause yet — or you may be in the very earliest stages where changes are minimal.
What to do:
Save this page. Bookmark it or print the checklists. Revisit in 6–12 months.
Start baseline awareness. Begin loosely tracking your cycles and any subtle changes. Having a baseline makes future comparisons much easier.
Don't dismiss your instincts. If something feels off, it's worth exploring — regardless of how many boxes you checked.
If You Checked 4–7 Boxes
Several signs consistent with perimenopause are present. This doesn't confirm a diagnosis, but it suggests your body may be beginning — or actively in — the hormonal transition.
What to do:
Track your symptoms for 4–8 weeks. Daily tracking reveals patterns that isolated observations miss. Note symptoms, cycle days, sleep quality, and stress levels.
Consider a doctor's appointment. Bring your completed checklist and your tracking data. Ask specifically whether perimenopause could explain your symptoms.
Request thyroid screening. Ask for TSH, Free T4, and thyroid antibodies — thyroid dysfunction mimics many perimenopause symptoms and becomes more common in your 40s.
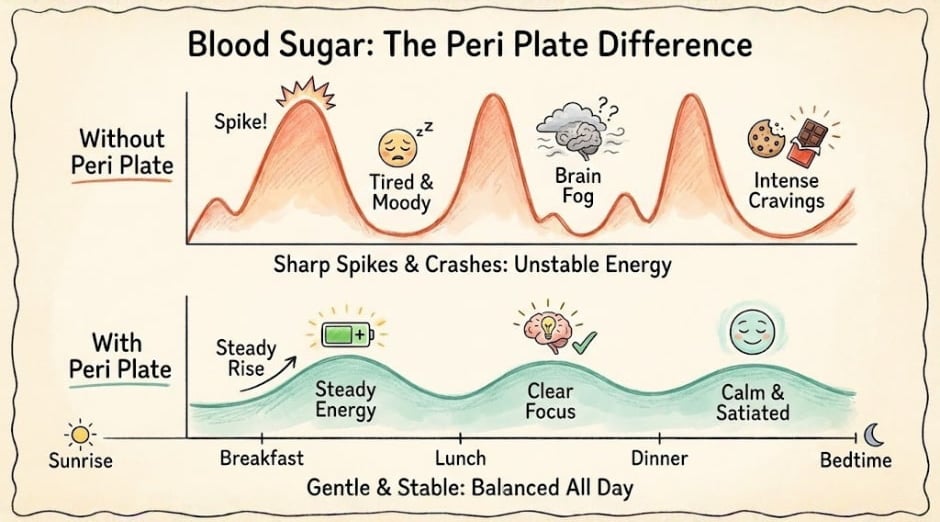
Start supportive lifestyle changes now. You don't need a formal diagnosis to prioritize protein, stabilize blood sugar, improve sleep hygiene, and manage stress.
If You Checked 8 or More Boxes
You're experiencing a significant symptom burden that aligns strongly with active perimenopause. Your body is very likely in the hormonal transition — and you deserve support.
What to do:
See a healthcare provider. Ideally, find a menopause-informed doctor or a NAMS-certified menopause practitioner. Come prepared with your checklist and tracking data.
Discuss treatment options. Hormone therapy, micronized progesterone, low-dose antidepressants, CBT-I for insomnia — there are effective, evidence-based options. You don't need to endure this unassisted.
Get a comprehensive health review. Bone density baseline, cardiovascular risk assessment, thyroid panel, iron/ferritin levels, vitamin D — perimenopause is a good time for a full health check.
Build your support system. Whether it's a knowledgeable friend, an online community, or a therapist who understands hormonal transitions — connection helps.
What to Bring to Your Doctor's Appointment
Preparation can transform a dismissive 10-minute appointment into a productive conversation.
Your appointment kit:
✅ Your completed checklist (from this page — print it or screenshot it)
✅ Your symptom tracking log (even 2–4 weeks of data helps)
✅ Your menstrual cycle history — any recent changes in length, flow, regularity
✅ A list of your top 3 concerns — ranked by impact on your quality of life
✅ Specific questions, such as:
"Could these symptoms be related to perimenopause?"
"Should we check my thyroid?"
"What treatment options would you recommend?"
"Would you consider referring me to a menopause specialist?"
✅ Your family history — when your mother/sisters went through menopause (if known)
Tools That Help You Track and Understand Your Symptoms
Why Tracking Matters More Than Testing
If blood tests can't reliably confirm perimenopause, your own data becomes your most powerful diagnostic tool.
Tracking does three things:
Reveals patterns you can't see in the moment — connecting symptoms to cycle phases, food, stress, and sleep
Validates your experience — seeing your symptoms documented in black and white makes them harder to dismiss (by you or anyone else)
Gives your doctor actionable information — a clear 4–8 week log is more clinically useful than a single hormone panel
What to track daily (takes 2–3 minutes):
Cycle day (if menstruating)
Sleep quality (1–5)
Energy level (1–5)
Mood (key emotions)
Physical symptoms (hot flashes, joint pain, headaches, palpitations)
Food/alcohol intake (brief notes)
Stress level (1–5)
🔎 Our Recommended Tracking Tools and Resources
This article may contain affiliate links. We only recommend products we've researched and believe may be genuinely useful for women in perimenopause. Affiliate commissions help support this site at no extra cost to you.
1. Balance App (by Dr. Louise Newson)
Best for: Women who want a free, menopause-specific symptom tracker with educational content
Why it helps: Developed by one of the UK's leading menopause specialists. Tracks symptoms, generates health reports you can share with your doctor, and provides evidence-based information
Strengths: Free, medically informed, produces a clear symptom summary for GP appointments
Limitations: UK-focused content (though universally useful for tracking)
2. The Perimenopause Journal — Daily Symptom & Cycle Tracker
Best for: Women who prefer pen-and-paper tracking or want a guided journaling approach
Why it helps: Structured daily pages combine symptom logging with brief reflective prompts — helping you connect patterns between your physical symptoms, mood, cycle, and lifestyle
Strengths: Tangible, no screen time required, encourages consistent tracking through guided format
Limitations: Not digital — patterns must be reviewed manually
3. Oura Ring (Gen 3)
Best for: Women who want objective sleep and temperature data to correlate with symptoms
Why it helps: Tracks sleep stages, heart rate variability (HRV), and body temperature trends — all of which shift during perimenopause. Temperature tracking can help identify ovulation patterns and hormonal fluctuations
Strengths: Objective biometric data, temperature trend analysis, excellent sleep tracking
Limitations: Investment cost ($299+), requires subscription for full features, doesn't diagnose perimenopause but provides valuable data
Scientifically relevant: Research shows that body temperature fluctuations correlate with vasomotor symptoms — tracking these can help identify patterns
4. "The New Menopause" by Dr. Mary Claire Haver
Best for: Women who want a comprehensive, accessible book on navigating perimenopause and menopause — including nutrition, HRT, and symptom management
Why it helps: Written by a board-certified OB-GYN who specializes in menopause. Combines medical evidence with practical guidance in an approachable tone. Covers what to ask your doctor, how to evaluate treatment options, and why you deserve better care
Strengths: Up-to-date research, practical protocols, empowering tone, covers the Galveston Diet approach for midlife nutrition
Limitations: One perspective — always complement with your own provider's guidance
5. Magnesium Glycinate Supplement (200–400 mg)
Best for: Women experiencing sleep disruption, anxiety, or muscle tension as part of perimenopause
Why it may help: Magnesium glycinate is the most bioavailable and gentle form of magnesium. It supports GABA activity (calming neurotransmitter), muscle relaxation, and sleep quality. Many women in perimenopause are magnesium-deficient without knowing it
What science says: Evidence for magnesium's role in sleep is modest but positive. It's not a guaranteed solution, but it's low-risk and well-tolerated for most people. A 2012 study in the Journal of Research in Medical Sciences found supplementation improved sleep quality in older adults
Strengths: Generally well-tolerated, affordable, widely available, may support multiple symptoms simultaneously
Limitations: Results vary individually. High doses can cause GI issues. Always check with your provider if you take other medications
Look for: Third-party tested brands (USP or NSF certified) — supplement quality varies significantly
Important YMYL note: No supplement replaces medical treatment for significant perimenopause symptoms. Magnesium may offer supportive benefit, but evidence is limited compared to interventions like hormone therapy or CBT-I. Individual results vary. Discuss supplementation with your healthcare provider.
You Deserve an Answer — Even If It's Not a Definitive One
Here's the truth that many health articles won't tell you:
You may never get a definitive, lab-confirmed, doctor-stamped diagnosis of perimenopause.
And that's okay. Because perimenopause isn't diagnosed like a disease — it's recognized like a season. You know autumn has arrived not because someone tests the air temperature, but because the leaves are changing, the light is shifting, and the mornings feel different.
Your body has its own signals. The checklists in this article are designed to help you read those signals clearly — to move from "am I imagining this?" to "I understand what's happening, and here's what I can do about it."
What matters most isn't a label. It's recognition.
Recognition that your symptoms are real. That they have a biological explanation. That you're not falling apart — you're transitioning. And that support is available if you want it.
You're not too young. You're not overreacting. And asking "Am I in perimenopause?" is one of the most important health questions you can ask yourself right now.
Trust the question. Trust the checklist. Trust your body.
FAQ — Am I in Perimenopause?
Q: At what age does perimenopause usually start?
A: Perimenopause typically begins in the mid-40s but can start as early as the late 30s. The transition lasts an average of 4–8 years before menopause, which occurs at an average age of 51.
Q: Can a blood test confirm I'm in perimenopause?
A: Not reliably. Hormone levels — especially FSH and estradiol — fluctuate dramatically during perimenopause, making single blood tests unreliable. Diagnosis is primarily clinical, based on symptoms, age, and menstrual changes.
Q: Can I be in perimenopause if I still have regular periods?
A: Yes. Many women experience perimenopause symptoms — mood changes, sleep disruption, anxiety — while still menstruating regularly. Progesterone often declines before cycle irregularity becomes visible.
Q: What's the difference between perimenopause and early menopause?
A: Perimenopause is the normal transition phase before menopause, typically starting in the 40s. Early menopause refers to menopause occurring before age 45. Premature ovarian insufficiency (POI) is menopause before 40 — a different medical condition.
Q: How do I know if my symptoms are perimenopause or thyroid problems?
A: Many symptoms overlap — fatigue, mood changes, weight shifts, cycle irregularities. A thyroid panel (TSH, Free T4, antibodies) can help differentiate. Both conditions can also coexist, so screening is recommended.
Q: Should I see a doctor if I think I'm in perimenopause?
A: Yes, especially if symptoms are affecting your quality of life. A menopause-informed provider can rule out other causes, validate your experience, and discuss treatment options including lifestyle changes and hormone therapy.
Perimenopause Compass
Contact
hello@perimenopausecompass.com
© 2026 All rights reserved.