Perimenopause vs Premature Ovarian Insufficiency (POI)
Perimenopause vs poi or premature ovarian insufficiency? The symptoms overlap, but the causes, timeline, and care are very different. Learn how to tell the difference — and why it matters.
EDUCATIONAL
3/4/202621 min read
You're 38. Your periods have become irregular. You're having night sweats. Your doctor orders blood tests and your FSH comes back elevated.
Is this perimenopause? Early menopause? Or something called premature ovarian insufficiency?
The answer changes everything — your treatment, your fertility options, your long-term health strategy, and your emotional experience. But the symptoms can look almost identical.
Perimenopause and premature ovarian insufficiency (POI) are two fundamentally different conditions that share many of the same symptoms. Confusing them — in either direction — can lead to years of mismanagement, unnecessary anxiety, or missed medical care.
This article draws the clearest possible line between the two. You'll learn what each condition actually is, how they differ in every clinically important way, how doctors should distinguish them, and what changes about your care depending on your diagnosis.
Whether you're wondering about your own symptoms, supporting someone who's been diagnosed, or trying to make sense of confusing test results — this is the resource that puts the full picture in one place.
Why This Distinction Matters More Than Most Women Realize
The Diagnostic Confusion That Costs Women Years
The confusion between perimenopause and POI is not a minor semantic issue. It creates real clinical harm in both directions:
When POI is missed and called "early perimenopause":
A 35-year-old woman with irregular periods and hot flashes is told she's "probably just starting perimenopause early" — reassured and sent home
In reality, her ovaries are failing prematurely — a condition that requires immediate HRT, bone density monitoring, cardiovascular risk management, and fertility counseling
Without this care, she faces accelerated bone loss, increased cardiovascular risk, and potential cognitive implications — all of which are largely preventable with appropriate treatment
She may also lose her fertility window without having the chance to explore preservation options
When perimenopause is misdiagnosed as POI:
A 42-year-old woman has a single elevated FSH reading and is told she has "premature ovarian failure"
She's devastated — told her ovaries have "failed," her fertility is gone, and she's heading toward menopause years early
In reality, her FSH is elevated because she's in normal early perimenopause — her ovaries are still functioning, she may still ovulate, and she has years of transition ahead
She spends months or years carrying the weight of a misdiagnosis that was based on a single unreliable blood test
Both scenarios happen every day in clinical practice. And both are preventable with better understanding.
What's at Stake When the Wrong Label Is Applied
Who Needs to Read This Article
Women under 40 experiencing menstrual irregularity, hot flashes, or unexplained symptoms
Women aged 40–45 whose doctors have mentioned "early menopause" or "premature ovarian failure" — terms that may be imprecisely applied
Women with elevated FSH who don't know what it means
Women recently diagnosed with POI who want to understand what it is and isn't
Any woman who wants to understand the difference — because knowledge is the foundation of good care
This article is for educational purposes and does not replace medical advice. Both perimenopause and POI require professional medical guidance. If you suspect either condition, consult a healthcare provider.
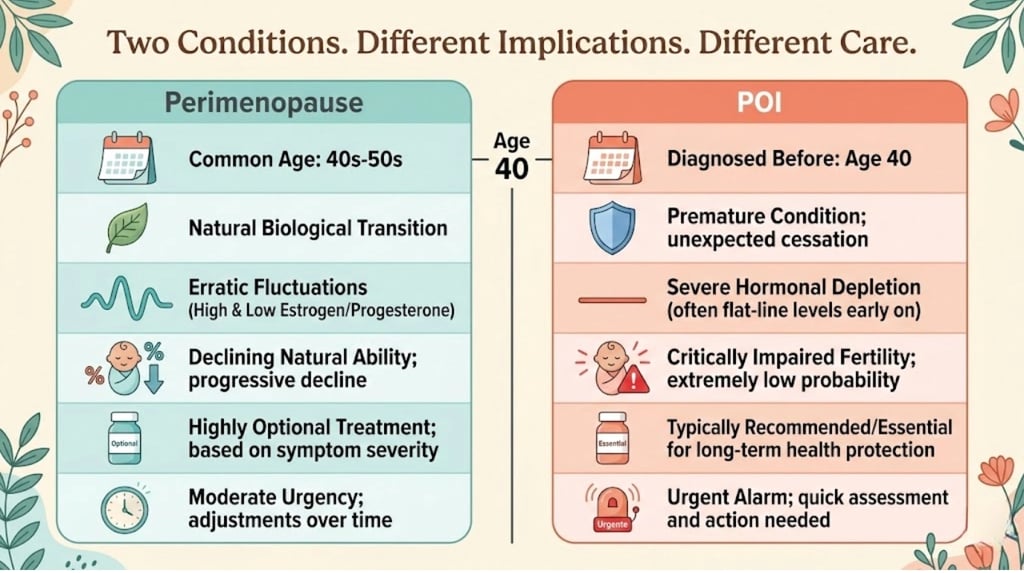
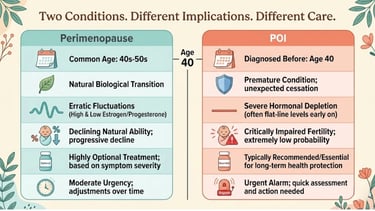
The Quick Comparison — Perimenopause vs POI at a Glance
The Summary Table
The One-Paragraph Distinction
Perimenopause is the normal, expected transition toward menopause that every woman experiences — typically beginning in the mid-40s and lasting 4–8 years, characterized by fluctuating (not just declining) hormones, gradually irregular periods, and a wide range of symptoms. Premature ovarian insufficiency (POI) is a medical condition in which the ovaries lose function before age 40 — causing estrogen deficiency, menstrual disruption, reduced fertility, and increased long-term health risks (bone, heart, brain) that require immediate medical attention and long-term hormone replacement.
What Is Perimenopause? (Brief Recap)
Definition and Normal Timeline
Perimenopause is the transitional phase when your ovaries gradually produce less estrogen and progesterone, ovulation becomes inconsistent, and your body moves toward the end of reproductive function.
Typical onset: Mid-40s (range: 38–early 50s)
Duration: Average 4–8 years (range: 2–12+)
Ends at: Menopause — defined as 12 consecutive months without a period (average age 51)
It's normal: Every woman with ovaries goes through perimenopause
Hormonal Profile of Perimenopause
The key hormonal characteristic of perimenopause is instability, not just decline:
Estrogen fluctuates wildly — spiking (sometimes to levels higher than your 20s) then crashing. This unpredictability drives most acute symptoms
Progesterone declines more steadily — because it's only produced after ovulation, and ovulation is becoming inconsistent
FSH rises as your pituitary tries harder to stimulate aging ovaries — but it's highly variable day to day
AMH (Anti-Müllerian Hormone) gradually decreases, reflecting declining ovarian reserve
Critical point: A single elevated FSH reading during perimenopause does NOT mean your ovaries have failed. It means your pituitary is working harder on that particular day. Tomorrow, it might be normal.
What Perimenopause Feels Like
The symptom experience of perimenopause is wide-ranging and well-documented across this site. In brief:
Irregular periods (shorter → longer → skipped)
Hot flashes and night sweats
Sleep disruption
Mood changes — anxiety, irritability, depression
Brain fog
Joint pain
Fatigue
Changes in libido
Weight redistribution
And many more — including the "obscure" somatic symptoms
The crucial characteristic: these symptoms emerge gradually, often over years, and the trajectory — while not linear — moves generally toward menopause.
What Is Premature Ovarian Insufficiency (POI)?
Definition — And Why the Name Changed
Premature ovarian insufficiency (POI) is a medical condition in which the ovaries lose their normal function before age 40 — leading to reduced estrogen production, irregular or absent periods, and impaired fertility.
The name change matters:
The older term — "premature ovarian failure" (POF) — has been largely replaced by "premature ovarian insufficiency" because:
"Failure" implies complete and permanent shutdown — which isn't accurate. Many women with POI have intermittent ovarian activity — occasional ovulation, unpredictable estrogen production, and even (rarely) spontaneous pregnancy
"Insufficiency" more accurately reflects the reality: ovarian function is insufficient and unreliable, but not necessarily entirely absent
The term change also reduces the psychological devastation of being told your ovaries have "failed" — language that many women describe as traumatic
Some medical resources and doctors still use "premature ovarian failure" or "premature menopause." If your doctor uses these terms, ask them to clarify whether they mean POI — and know that the modern, more accurate term is premature ovarian insufficiency.
POI vs Early Menopause vs Premature Menopause — Clearing Up the Terms
These terms overlap and are often used interchangeably — incorrectly. Here's the precise distinction:
The key clinical distinction:
POI (before 40) is a medical condition requiring investigation, treatment, and monitoring
Early menopause (40–45) is at the early end of normal — may not require the same level of investigation, but does warrant earlier bone and cardiovascular attention
Normal menopause (45–58) is expected and managed symptomatically
If you reached menopause before 40: You have POI (or premature menopause). This is NOT normal perimenopause — it requires specific medical care.
If you reached menopause between 40–45: You have early menopause. This is within the normal range but at the early end — discuss HRT and screening with your provider.
How Common Is POI?
POI affects approximately:
1 in 100 women under age 40
1 in 1,000 women under age 30
1 in 10,000 women under age 20
While these numbers may seem small, they represent hundreds of thousands of women worldwide. And because POI is frequently misdiagnosed or diagnosed late, the actual prevalence may be higher.
Causes of POI — Known and Unknown
Important for autoimmune POI: Women with POI should be screened for coexisting autoimmune conditions — particularly thyroid autoimmunity (present in approximately 20–30% of POI cases) and adrenal insufficiency (rare but serious). These screenings are part of standard POI workup per ESHRE guidelines.
The Hormonal Profile of POI
The hormonal picture in POI is different from perimenopause:
The critical hormonal difference: In perimenopause, hormones fluctuate wildly. In POI, estrogen is consistently low (with occasional, unpredictable returns of function). This distinction is why a single blood test can't distinguish between them — you need repeated testing over time.
What POI Feels Like — And How It Differs from Perimenopause
Many POI symptoms are identical to perimenopause — because both involve estrogen deficiency:
Irregular or absent periods
Vaginal dryness
Sleep disruption
Mood changes
Brain fog
Fatigue
But the experience of POI often differs in several important ways:
The onset is often more abrupt:
While perimenopause creeps in gradually over years, POI often presents more suddenly — a woman in her 30s whose periods simply stop, or become very irregular within months rather than years.
The emotional impact is different:
A 47-year-old entering perimenopause may feel frustrated, but she's experiencing something expected for her age. A 34-year-old diagnosed with POI is facing something unexpected, premature, and potentially devastating — particularly if she wanted children or hadn't finished building her family.
The medical urgency is different:
Perimenopause is a transition to manage. POI is a condition to treat — because the years of estrogen deficiency ahead carry significant health risks that aren't present when menopause occurs at the normal age.
The identity impact is different:
Many women with POI describe a profound sense of loss — not just of fertility, but of their place in their life stage. Being told your reproductive years are over in your 30s, when peers are having babies, can create an isolation that's qualitatively different from the perimenopause experience.
Side-by-Side Comparison — Every Key Difference
Age of Onset
The age-40 threshold is the most important clinical dividing line:
After 40: Menstrual irregularity and elevated FSH are most likely perimenopause — a normal transition
Before 40: The same symptoms require POI investigation — because ovarian failure at this age is NOT normal and has different implications
Hormonal Pattern
Menstrual Changes
Symptom Profile
Fertility Implications
Bone and Cardiovascular Risk
This is where the distinction has the most serious long-term health implications:
The critical research:
The Nurses' Health Study found that women with menopause before age 40 had significantly higher cardiovascular mortality compared to women with menopause at the normal age
A meta-analysis in BJOG found that POI is associated with a 50% increased risk of cardiovascular disease and significantly increased risk of osteoporosis
These risks are largely mitigated by appropriate HRT — which is why HRT for POI is not optional but medically indicated
Diagnosis
Treatment Approach
Emotional and Psychological Impact
The emotional experience of POI deserves special emphasis because it is qualitatively different from the perimenopause experience — and it is frequently underestimated by healthcare providers.
A 35-year-old woman diagnosed with POI isn't just managing hot flashes. She's potentially:
Mourning the children she may not have
Feeling disconnected from friends who are pregnant or breastfeeding
Processing a medical reality that she didn't expect for another 15 years
Questioning her femininity, desirability, and identity
Managing physical symptoms while also managing profound emotional upheaval
This is not the same experience as perimenopause. And it should not be treated as such — by doctors, by partners, or by support resources.
The Master Comparison Table
What Women Actually Experience
"I Was 36. They Told Me It Was Stress."
"My periods stopped at 36. I went to my GP who said it was 'probably stress' — I'd just changed jobs. Six months passed. No period. I went back. He tested my thyroid. Normal. He said 'give it time.' Another six months. Still nothing. Finally, a different GP tested my FSH: 78. She went quiet and said: 'Your ovaries aren't functioning normally. This is premature ovarian insufficiency.' I was 37 by then. Thirteen months of dismissal. Thirteen months of bone loss and cardiovascular risk accumulating without treatment. Thirteen months I'll never get back — and during which my remaining fertility further declined."
"I Thought POI Meant My Life Was Over"
"When my gynecologist said 'premature ovarian failure,' I heard: you're broken. You'll never have children. You're menopausal at 33. Your body has failed. I went home and cried for three days. What I wish she'd said instead: 'Your ovaries aren't working as expected right now. There's a small chance of intermittent function and even pregnancy. We're going to protect your bones and heart with hormones, and I'm referring you to a fertility specialist to discuss your options. You're going to be okay — this is manageable.' Language matters. The word 'failure' almost broke me more than the condition itself."
"My Perimenopause Was Misdiagnosed as POI — And I Spent a Year Terrified"
"At 42, I had a single FSH test that came back at 35. My doctor said: 'It looks like premature ovarian failure.' She referred me to a reproductive endocrinologist and told me to prepare for menopause. I was devastated. The RE did a proper workup — repeated FSH (which came back at 18 the second time), checked my AMH (low-normal, not undetectable), did an ultrasound (small but visible follicles). She looked at me and said: 'You're 42. This is perimenopause. Your first FSH was just a snapshot on a bad day. You don't have POI.' The relief was indescribable. But I'd spent a year believing my ovaries had failed — a year of grief, anxiety, and fear — because of a single misinterpreted blood test."
"Getting the Right Diagnosis Changed Everything"
"I was diagnosed with POI at 38 — properly, by a reproductive endocrinologist, with two elevated FSH tests, an undetectable AMH, and a karyotype that showed a genetic variant. Instead of panic, I got a plan: HRT to protect my bones and heart, a referral to a fertility clinic to discuss egg donation, a DEXA scan baseline, and a connection to a POI support community. The diagnosis was hard. But the right diagnosis, with the right care team, made it feel manageable. I now know exactly what I need, why I need it, and who to turn to. That's the difference between a label and a diagnosis."


What Science Says — How Doctors Distinguish Between the Two
The FSH Test — What It Shows and What It Doesn't
FSH (Follicle-Stimulating Hormone) is the most commonly used blood test in this context — and the most commonly misinterpreted.
What FSH actually measures:
FSH is produced by your pituitary gland to stimulate your ovaries to produce follicles (and therefore estrogen). When your ovaries respond less, your pituitary produces more FSH — like turning up the volume because the speaker isn't responding.
In perimenopause:
FSH is highly variable — it can be 15 one week and 55 the next
A single elevated reading does NOT confirm anything — it's a snapshot of a fluctuating system
FSH can be elevated one month and normal the next because the ovaries are still intermittently responsive
UK NICE guidelines explicitly state that FSH testing is not required to diagnose perimenopause in women over 45
In POI:
FSH is consistently elevated — ≥25 IU/L (some guidelines use ≥40 IU/L) on two separate occasions, at least 4–6 weeks apart
The consistency is the key — both readings should be elevated, not just one
This indicates the ovaries are persistently unresponsive to pituitary stimulation
The diagnostic error to avoid:
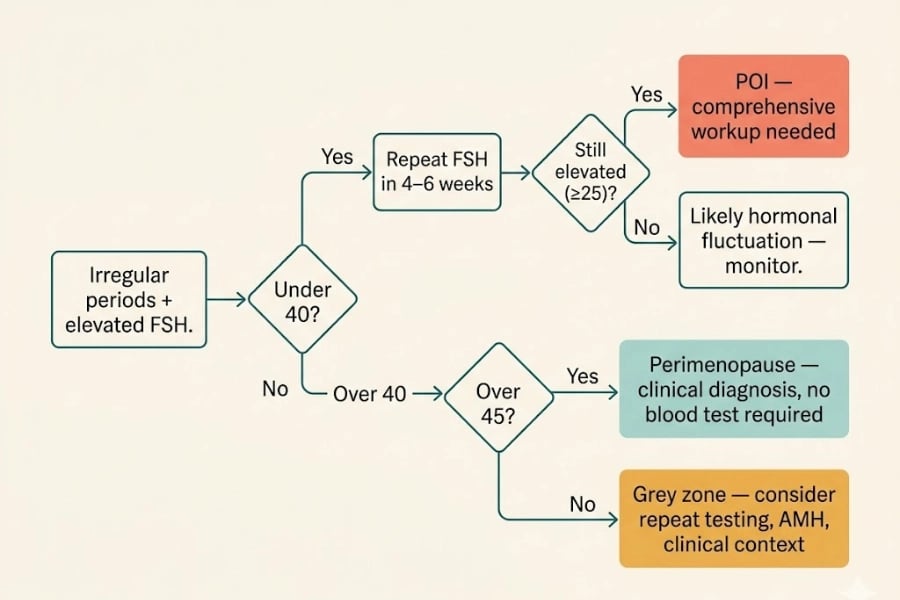
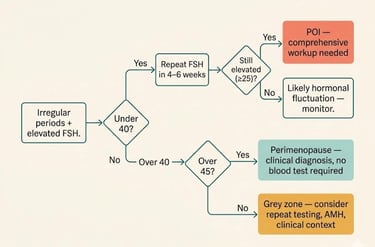
A single elevated FSH in a woman over 40 → perimenopause, not POI
A single elevated FSH in a woman under 40 → warrants retesting before any diagnosis is made
AMH (Anti-Müllerian Hormone) — A Better Marker?
AMH reflects your ovarian reserve — the number of remaining follicles capable of developing.
Advantage of AMH: It's more stable than FSH — it doesn't fluctuate with the menstrual cycle, making it a more reliable single measurement.
Limitation: There's no universally agreed AMH cutoff for POI. Very low or undetectable AMH in a woman under 40 is strongly suggestive, but AMH alone doesn't make the diagnosis.
The ESHRE Diagnostic Criteria for POI
The European Society of Human Reproduction and Embryology (ESHRE) published the gold-standard diagnostic guidelines for POI in 2016. The criteria are:
POI is diagnosed when ALL THREE are present:
Age — under 40
Menstrual disruption — oligomenorrhea (infrequent periods) or amenorrhea (absent periods) for ≥4 months
Elevated FSH — ≥25 IU/L on two measurements, taken at least 4–6 weeks apart
Additional recommended investigations (per ESHRE):
Karyotype — to check for Turner syndrome or other chromosomal causes
Fragile X premutation screening — associated with POI
Adrenal antibodies (21-hydroxylase) — to assess for autoimmune adrenal insufficiency (Addison's)
Thyroid antibodies + TSH — to screen for coexisting autoimmune thyroid disease
DEXA scan — baseline bone density
Pelvic ultrasound — to assess ovarian size and antral follicle count
Why the ESHRE criteria matter:
They establish that POI diagnosis requires more than one test — protecting against the single-FSH-snapshot misdiagnosis. They also mandate comprehensive screening for associated conditions — which is essential because POI is often part of a broader autoimmune picture.
Why Diagnosis Requires More Than One Blood Test
This point cannot be overemphasized:
You cannot diagnose POI on a single blood test. And you cannot diagnose perimenopause on a single blood test.
In perimenopause, FSH fluctuates so wildly that a single reading is clinically meaningless
In POI, the diagnosis requires two elevated readings separated by 4–6 weeks — to confirm consistency
AMH provides additional context but doesn't make the diagnosis alone
Clinical context (age, symptoms, menstrual history, family history) is essential
If you've been given a diagnosis — POI or perimenopause — based on a single blood test, ask your provider to confirm with repeat testing and a comprehensive evaluation.
Established vs. Evolving Understanding
Scientifically established:
POI is defined by ovarian dysfunction before age 40 with elevated FSH (≥25 IU/L × 2)
POI is associated with increased cardiovascular mortality, osteoporosis, and possible cognitive risk
HRT is medically indicated for POI at least until average menopause age
~50–60% of POI cases are idiopathic (cause unknown)
Autoimmune mechanisms account for 20–30% of cases
5–10% of POI women experience spontaneous pregnancy
Perimenopause is clinically diagnosed and doesn't require blood tests in women over 45
Probable (growing evidence):
Some cases of "idiopathic" POI may involve environmental endocrine disruptors
Genetic testing may eventually identify many more causative variants
The cardiovascular risk of POI may be partly independent of estrogen deficiency (other ovarian factors may contribute)
Intermittent ovarian function in POI may be more common than previously thought
Still debated or under-researched:
Optimal HRT dosing for POI (physiological replacement vs. standard menopausal doses)
Whether the combined OCP is equivalent to HRT for bone protection in POI
Long-term cognitive outcomes in POI with and without HRT
Whether new fertility technologies will improve own-egg IVF outcomes in POI
The role of the gut microbiome and inflammation in autoimmune POI
Can POI Be Mistaken for Perimenopause? (And Vice Versa)
When Perimenopause Starts Early — The Grey Zone
Some women enter perimenopause in their late 30s — which creates a diagnostic grey zone:
She's 39, periods are becoming irregular, FSH is elevated on one test
Is this early-normal perimenopause? Or is it POI presenting at the upper age boundary?
How to distinguish:
Repeat FSH testing — if it's consistently ≥25 IU/L on two occasions, POI criteria are met (she's still under 40)
AMH testing — very low or undetectable AMH in a woman under 40 supports POI
Clinical trajectory — perimenopause evolves gradually; POI often (though not always) progresses more rapidly
Family history — early menopause in mother/sisters may suggest genetic predisposition (could be either early perimenopause or POI)
Autoimmune history — personal or family history of autoimmune disease raises POI suspicion
When POI Presents Mildly — The Missed Diagnosis
Not all POI presents dramatically. Some women with POI:
Still have occasional periods (oligomenorrhea rather than amenorrhea)
Have mild symptoms that are easily attributed to stress or lifestyle
Are on hormonal contraception that masks menstrual changes
Are not trying to conceive and therefore not aware of fertility issues
In these cases, POI can go undiagnosed for years — during which bone density and cardiovascular risk silently worsen.
Who should be screened for POI even without classic presentation:
Women under 40 with 4+ months of irregular or absent periods (not explained by pregnancy, contraception, or other conditions)
Women under 40 with unexplained infertility
Women with autoimmune conditions (especially thyroid) who develop menstrual changes
Women with a family history of POI or early menopause
Women who have undergone chemotherapy or pelvic radiation
The Age 40 Threshold — Why It Matters Clinically
Age 40 is the clinical dividing line — not because biology changes overnight at 40, but because the medical framework changes:
The threshold exists because the consequences differ:
A woman who loses ovarian function at 38 has 13+ years of estrogen deficiency ahead before the "normal" menopause age — years during which bone loss and cardiovascular risk accumulate without treatment
A woman who enters perimenopause at 44 has a much shorter window of deficiency — and a lower cumulative risk
Long-Term Health Implications — Why the Correct Diagnosis Is Critical
Bone Density and Osteoporosis Risk
Estrogen is the primary protector of bone density in women. It supports osteoblast activity (building bone) and inhibits osteoclast activity (breaking bone down).
In perimenopause: Bone loss begins during the transition and accelerates after menopause — with the most rapid loss in the first 5–7 years postmenopause.
In POI: Bone loss begins much earlier — potentially in the 20s or 30s. By the time a woman with untreated POI reaches 50, she may have the bone density of a woman in her 60s or 70s.
Clinical implications:
Women with POI should have a DEXA scan at diagnosis — not at menopause age
HRT is essential for bone protection — not optional
Weight-bearing exercise, calcium (1,200 mg/day), and vitamin D are critical adjuncts
Bone density should be monitored every 2–3 years
Cardiovascular Health
Estrogen is cardioprotective — it supports healthy cholesterol profiles, blood vessel flexibility, and anti-inflammatory vascular function.
In POI:
Cardiovascular disease risk is significantly increased
The Nurses' Health Study found that menopause before 40 is associated with higher cardiovascular mortality
A 2019 meta-analysis in European Heart Journal confirmed increased cardiovascular risk in women with POI
This risk is largely reversible with HRT — making treatment not just symptom management but cardiovascular prevention
In perimenopause: Cardiovascular risk increases gradually — and HRT may offer protection when started within 10 years of menopause onset (the "timing hypothesis").
Cognitive and Neurological Considerations
Estrogen supports neuronal health, synaptic plasticity, and neuroprotection. Emerging research suggests:
Early estrogen deficiency (as in POI) may be associated with earlier cognitive decline — though evidence is not yet definitive
The timing hypothesis suggests that estrogen replacement closer to the time of ovarian failure may be more neuroprotective than replacement started years later
HRT in POI may therefore have neuroprotective value — though this is an active area of research
In perimenopause: Cognitive changes (brain fog, memory lapses) are well-documented but typically temporary — resolving after menopause as hormones stabilize.
Fertility and Family Planning
In perimenopause: Fertility is declining but natural conception remains possible. Most women in perimenopause are not primarily concerned about fertility.
In POI: Fertility is the most emotionally charged aspect of the diagnosis:
Own-egg IVF has very low success rates in POI (because the core problem is depleted egg supply)
Egg donation IVF offers much higher success rates and is the most common assisted reproduction option for women with POI
Spontaneous pregnancy occurs in approximately 5–10% of POI cases — unpredictably. This means contraception should be discussed if pregnancy is not desired
Fertility preservation (egg freezing) may be discussed if some ovarian function remains — but success depends on the degree of remaining function
Adoption and surrogacy are alternative pathways that some women explore
The urgency: If a woman with POI desires biological children, time is critical — referral to a reproductive endocrinologist should happen at diagnosis, not months later.
Psychological Wellbeing
The psychological impact of POI is distinct and significant:
Grief — for the reproductive future that may not happen
Identity disruption — "menopause" in your 30s challenges fundamental assumptions about your body, your womanhood, and your life timeline
Relationship stress — particularly around fertility, intimacy, and the partner's response
Social isolation — peers are not going through this, support groups are small, awareness is low
Stigma and shame — internalized messages about "broken" bodies, "failed" ovaries
Anxiety — about long-term health consequences, treatment decisions, and the uncertainty of intermittent ovarian function
Clinical implication: Psychological support should be part of the standard POI care package — not an afterthought. This may include individual therapy, couples counseling, peer support groups, and connection to POI-specific communities.
Treatment Differences — What Changes Depending on Your Diagnosis
HRT for Perimenopause vs HRT for POI — Not the Same Conversation
This is a crucial distinction that many providers blur:
The WHI data context:
The Women's Health Initiative (WHI) study — which raised concerns about HRT risks — studied older postmenopausal women (average age 63). Its findings do not apply to young women with POI who are replacing physiologically necessary hormones. ESHRE and NAMS guidelines are clear: HRT for POI carries a different — and much more favorable — risk-benefit profile than elective HRT in older women.
Any provider who refuses HRT to a woman with POI citing WHI data is misapplying the evidence. This is a situation where advocacy and, if necessary, a second opinion are essential.
Fertility Preservation and Options in POI
Key message: The conversation about fertility should happen at diagnosis — even if the woman is not currently planning children. Knowing the options, the limitations, and the timelines empowers informed decision-making.
Bone and Heart Protection Protocols
Psychological Support and Community
🔎 Recommended Resources
This article may contain affiliate links. We only recommend products we've researched and believe may be genuinely useful. Affiliate commissions help support this site at no extra cost to you.
1. "The Menopause Manifesto" by Dr. Jen Gunter
Best for: Comprehensive understanding of both perimenopause and premature ovarian insufficiency — including the medical, hormonal, and emotional dimensions
Why it helps here: Dr. Gunter covers POI specifically and discusses the evidence for HRT in young women with clarity. Excellent for both conditions
2. "The Complete Guide to POI and Early Menopause" by Dr. Hannah Short and Dr. Mandy Leonhardt
Best for: Women newly diagnosed with POI — or those who suspect it
Why it helps here: One of the only books written specifically about POI — covers medical management, fertility options, emotional support, and long-term health in accessible language. Written by menopause specialists
3. Balance App (by Dr. Louise Newson)
Best for: Symptom tracking and health reports — useful for both perimenopause and POI management
Why it helps here: Tracks symptoms over time, generating reports that support medical consultations. Useful for documenting your experience regardless of diagnosis
4. Vitamin D3 + K2 Supplement
Best for: Bone protection — critical for both perimenopause and especially POI
Why it helps here: Vitamin D deficiency is very common and directly affects bone health. In POI, where bone protection is urgent, optimizing vitamin D is essential. K2 directs calcium to bones
Evidence level: Strong — well-established for bone health
Important: Test vitamin D levels before supplementing. Target: 50–80 nmol/L (UK) / 40–60 ng/mL (US)
YMYL disclosure: No book, app, or supplement replaces medical evaluation and treatment for POI. POI requires professional management — ideally by a reproductive endocrinologist or menopause specialist. These resources support, but do not replace, clinical care.
How to Get the Right Diagnosis
What to Ask Your Doctor
If you're under 40 with menstrual irregularity:
"Could this be premature ovarian insufficiency? I'd like to check my FSH levels."
"If FSH is elevated, can we repeat the test in 4–6 weeks to confirm?"
"Can we also check my AMH level?"
"Should I be screened for autoimmune conditions — particularly thyroid antibodies?"
"If POI is confirmed, I'd like a referral to a reproductive endocrinologist and a baseline DEXA scan."
If you're between 40–45 with an elevated FSH:
"Is this perimenopause, or should we investigate for POI?"
"Was this a single FSH test? Should it be repeated?"
"What was my AMH level?"
"Do I need any additional screening?"
"What does this mean for my bone and heart health?"
If you're over 45 with menstrual changes:
"I understand this is likely perimenopause. Blood tests aren't needed to confirm, correct?"
"Can we focus on symptom management and discuss HRT options?"
The Tests That Matter
When to Seek a Specialist
Reproductive endocrinologist — for fertility counseling, diagnosis confirmation, and treatment planning
Menopause specialist (NAMS-certified) — for HRT optimization and long-term management
Genetic counselor — if genetic causes are identified (Fragile X, Turner syndrome)
Endocrinologist — if autoimmune conditions are coexisting (thyroid, adrenal)
Psychologist/therapist — for emotional processing, grief work, relationship support
Building Your Diagnostic Case
If you suspect POI and are struggling to get appropriate investigation:
Document your menstrual history — dates, gaps, changes over time
List your symptoms — organized by system (use our body systems framework)
Note your age — emphasize that you are under 40 and that menstrual disruption at this age warrants investigation
Cite ESHRE guidelines — you can reference the criteria: "ESHRE recommends FSH testing on two occasions 4–6 weeks apart, plus comprehensive screening, for women under 40 with menstrual disruption"
Request specific tests — FSH, estradiol, AMH, thyroid antibodies
Ask for referral if your GP is uncertain — a reproductive endocrinologist is the appropriate specialist
If You've Just Been Diagnosed with POI — What to Know First
If you're reading this section because you've recently received a POI diagnosis, here's what we want you to hear first:
You are not broken. POI is a medical condition — not a personal failure. Your ovaries didn't fail because of something you did or didn't do.
Your diagnosis is not a death sentence for your hopes. Whether those hopes involve children, intimacy, health, or simply living fully — there are paths forward. They may look different from what you planned. But they exist.
HRT is your friend, not your enemy. You're not taking "extra" hormones. You're replacing hormones your body should be producing. This is not the same conversation as elective HRT after menopause. Taking HRT protects your bones, your heart, and your brain — and it can transform how you feel day to day.
You are not alone. POI communities exist — Daisy Network, online support groups, social media spaces. Finding women who understand this specific experience can be profoundly healing.
Your emotions are valid. Grief, anger, confusion, fear, relief (at finally having a name for it), numbness — all of these are normal responses. There is no correct way to feel. And professional support is not weakness — it's wisdom.
You can still live a full, vital, healthy life. With appropriate treatment, monitoring, and support, women with POI go on to have careers, relationships, families (through various pathways), and decades of good health. POI changes the route. It doesn't determine the destination.
Two Different Journeys — Both Deserve Understanding and Support
Perimenopause and POI are not the same journey. One is a normal transition that every woman navigates. The other is a medical condition that a smaller number of women face — earlier than expected, with different implications and different needs.
But they share something important: both involve a body in hormonal flux, a woman seeking answers, and a medical system that too often provides too little information, too late.
If this article has given you clarity — about which condition applies to you, about what to ask your doctor, about what the numbers mean, about what the differences are — then it's done its job.
If you're in perimenopause: You're navigating a normal, if challenging, transition. Support exists, treatment exists, and the transition has an end.
If you have POI: You're navigating a medical condition that arrived before its time. Treatment is essential, support is available, and your future is not defined by your diagnosis.
Both of you deserve:
A healthcare provider who understands the distinction
The right diagnosis, based on proper investigation
Access to appropriate treatment — without judgment, delay, or dismissal
Emotional support that matches the specific nature of your experience
The knowledge that you are not alone
FAQ — Perimenopause vs POI
Q: What is the difference between perimenopause and POI?
A: Perimenopause is the normal transition toward menopause, typically starting in the mid-40s. POI (premature ovarian insufficiency) is a medical condition where ovarian function declines before age 40. Both cause similar symptoms, but POI requires immediate treatment, bone/heart monitoring, and fertility counseling.
Q: At what age is menopause considered premature?
A: Menopause before age 40 is classified as premature (POI). Menopause between ages 40–45 is considered "early" but within the broader normal range. Menopause at 45–58 is considered normal, with 51 being the average.
Q: Can POI be mistaken for perimenopause?
A: Yes — and this happens frequently. A woman under 40 with irregular periods may be told she's "starting perimenopause early" when she actually has POI. Proper diagnosis requires two elevated FSH tests 4–6 weeks apart, not a single blood draw.
Q: Is POI the same as early menopause?
A: Not exactly. POI specifically refers to ovarian insufficiency before age 40 — and unlike complete menopause, intermittent ovarian function and even spontaneous pregnancy can occur. "Early menopause" more broadly refers to menopause between 40–45.
Q: Can you have children with POI?
A: Approximately 5–10% of women with POI conceive spontaneously. Egg donation IVF offers higher success rates. If biological children are desired, urgent referral to a reproductive endocrinologist is recommended at the time of diagnosis.
Q: Does POI require HRT?
A: Yes. HRT for POI is medically necessary — not optional — to protect bone density, cardiovascular health, and potentially cognitive function. It should continue at least until the average age of natural menopause (51). The risk-benefit profile is very different from elective HRT in older women.
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References
Perimenopause Compass
Contact
hello@perimenopausecompass.com
© 2026 All rights reserved.