Low Libido During Perimenopause: Causes and Support
Low libido during perimenopause is common, biological, and not your fault. Understand the real causes — hormonal, physical, and emotional — and find support that actually helps.
LIFESTYLE
Perimenopause Compass
2/22/202623 min read
When did you last want sex — not out of obligation, not to keep the peace, not because it had been "too long" — but because you genuinely, spontaneously desired it?
If you had to think for more than a few seconds, you're not alone. And if the answer brought a wave of guilt, confusion, or grief — you're especially not alone.
Low libido during perimenopause is one of the most common symptoms women experience — and one of the least discussed. It lives in the space between "I still love my partner" and "I just don't want to be touched." It's surrounded by shame, silence, and the persistent cultural message that something is wrong with you if your desire has faded.
Nothing is wrong with you.
Your libido is changing because your body is changing — hormonally, neurologically, and physically. And when you understand why, the path to support becomes much clearer.
This article covers all the causes of low libido during perimenopause — not just hormones — and offers practical, evidence-based, shame-free guidance for navigating this shift. Whether you want to reignite desire, redefine intimacy, or simply understand what's happening, this is the resource you deserve.
The Conversation Nobody's Having
Why Low Libido in Perimenopause Feels So Isolating
Of all perimenopause symptoms, low libido may be the most privately suffered.
Women talk about hot flashes. They joke about brain fog. They commiserate about insomnia. But desire? Sex? The quiet disappearance of something that used to be part of who you are?
That conversation happens in whispers — if it happens at all.
The isolation comes from multiple directions:
Cultural pressure: Women are expected to be sexually available, desirable, and enthusiastic. When desire fades, it's easy to feel like you've failed at femininity.
Relationship fear: Many women worry that admitting low desire will hurt their partner, threaten their relationship, or create conflict they don't have the energy for.
Medical dismissal: Women who raise libido concerns with their doctor are frequently met with shrugs, awkward silences, or "that's normal at your age" — which is neither helpful nor entirely accurate.
Comparison trap: Social media and cultural narratives present midlife women as sexually empowered and "in their prime" — which can make you feel even more broken if that's not your experience.
Here's the truth: low libido during perimenopause affects an estimated 40–55% of women during the menopausal transition. It's not rare. It's not abnormal. And it's absolutely worth addressing — whether "addressing" means finding solutions, finding acceptance, or finding a new definition of intimacy.
What This Article Will — And Won't — Do
This article will:
Explain every category of cause — hormonal, physical, neurological, relational, and medication-related
Share real women's experiences without sensationalizing
Present evidence-based options — from medical treatments to relationship strategies
Help you have better conversations with your partner and your doctor
Offer a framework for redefining intimacy on your own terms
This article will not:
Tell you there's something wrong with you
Promise to "fix" your libido
Suggest that desire should look the way it did at 25
Pressure you into wanting sex more than you want it
This article is for educational purposes and does not replace medical advice. Sexual health is personal and complex — consult a healthcare provider for guidance tailored to your individual situation.
What "Low Libido" Actually Means During Perimenopause
The Difference Between Desire, Arousal, and Pleasure
These three things are related but distinct — and understanding the difference changes how you think about your experience:
During perimenopause, any combination of these can change:
You may have reduced desire but still experience arousal and pleasure once engaged
You may have desire but reduced physical arousal (less lubrication, slower response)
You may have both desire and arousal but reduced pleasure (diminished sensation, difficulty reaching orgasm)
Or all three may shift simultaneously
Knowing which component has changed helps you — and your healthcare provider — target the right support.
Spontaneous vs. Responsive Desire — A Game-Changing Distinction
This is the concept that transforms how most women understand their libido — and it comes from sex researcher Dr. Emily Nagoski's groundbreaking work:
Spontaneous desire = desire that appears "out of nowhere" — you suddenly want sex without any specific trigger. This is what our culture treats as "normal" libido.
Responsive desire = desire that emerges in response to stimulation, context, and connection. You didn't necessarily want sex beforehand, but once the right conditions are created, desire follows.
Here's the crucial insight: Research suggests that approximately 70% of women experience primarily responsive desire — even before perimenopause. It's not a dysfunction. It's a completely normal pattern of female sexuality.
During perimenopause, spontaneous desire often decreases — because testosterone (which fuels spontaneous desire) is declining, and because your brain is occupied with managing a hundred other hormonal challenges.
But responsive desire — the kind that emerges when you feel safe, connected, rested, and gently aroused — can remain fully intact.
This means: the "I never think about sex anymore" experience doesn't necessarily mean your capacity for desire or pleasure is gone. It may mean the pathway to desire has changed — from spontaneous to responsive. And that's not a loss. It's a shift that can be worked with.
When It's a Shift vs. When It's a Problem
Low libido is a concern worth addressing when:
It causes you personal distress — you miss your desire, you feel disconnected from yourself
It creates relationship tension — mismatched desire is causing conflict or distance
It's accompanied by physical symptoms that make sex uncomfortable or painful (vaginal dryness, pain during intercourse)
It's accompanied by mood symptoms (depression, anxiety) that are affecting your overall quality of life
You want to feel more desire — and you'd like support getting there
Low libido is not inherently a problem if:
You feel content with your current level of sexual interest
Your relationship is not strained by the change
The shift doesn't cause you personal distress
You've consciously chosen to prioritize other forms of intimacy
There is no "correct" amount of desire. The question isn't whether your libido matches someone else's standard. The question is whether it matches yours.
What Women Actually Experience
"I Still Love My Partner — I Just Don't Want Sex"
"This is the hardest thing to explain. My husband is wonderful. Attractive. Kind. Present. I'm deeply in love with him. And I could happily go months without sex. Not because anything is wrong between us — but because the physical drive just… evaporated. It happened gradually. At first I thought I was just tired. Then I thought we'd lost our spark. Then I realized: this is my body. Something hormonal has shifted. And recognizing that — separating desire from love — was both a relief and a grief."
"I Don't Even Think About It Anymore"
"I used to think about sex. Not constantly, but it was there — a background hum of awareness. Some time in my mid-40s, that hum went silent. It wasn't that I decided not to want sex. It's that the thought stopped occurring to me. Like a radio station that went off the air. I didn't notice it disappearing — I noticed the silence. And then I felt guilty about not missing it sooner."
"It's Not Just Desire — Everything Feels Different Physically"
"People talk about low libido like it's just a mental thing — you don't want to. But for me, it's physical too. Things that used to feel good don't feel the same. I'm drier. I'm less sensitive. Orgasms are harder to reach and less intense when they happen. Sex went from something I enjoyed to something that requires effort, negotiation, and lube. It's not that I don't want connection. It's that my body doesn't cooperate the way it used to."
"The Guilt Is Almost Worse Than the Symptom"
"I feel guilty for not wanting sex. I feel guilty for how it affects my partner. I feel guilty for sometimes just going through the motions. I feel guilty for not feeling guilty enough to do something about it. And underneath all that guilt is this quiet anger: why does nobody talk about this? Why did nobody warn me? Why is the expectation that I should just carry on as normal when nothing about my body feels normal right now?"
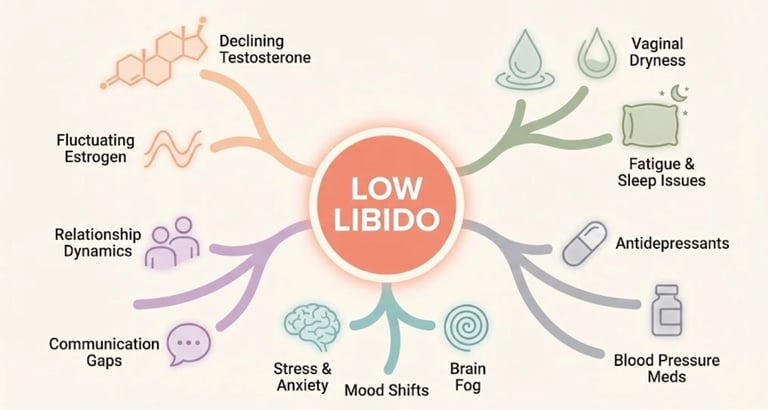
The Causes — Why Libido Changes During Perimenopause
Low libido during perimenopause is almost never caused by one thing. It's a convergence of multiple factors — hormonal, physical, neurological, relational, and sometimes medication-related — that interact and amplify each other.
Understanding all of them gives you the most accurate picture — and the most options for support.
Hormonal Causes
Declining Testosterone
This is the cause most people don't know about — because testosterone is perceived as a "male" hormone. But women produce testosterone too, and it plays a central role in sexual desire.
What's happening:
Women's testosterone levels begin declining from the late 20s to early 30s — well before perimenopause
By the time you reach your mid-40s, your testosterone may be approximately half of what it was at 20
Testosterone fuels spontaneous desire — the unprompted "I want sex" feeling
It also supports genital sensitivity, arousal response, and energy
The diagnostic challenge: Testosterone levels in women are measured in very small amounts, and there's no well-established "normal range" for female testosterone relative to sexual function. This means:
Blood tests may come back "normal" even when testosterone has dropped significantly from your personal baseline
Many doctors don't test testosterone in women at all
Even when they do, they may not know how to interpret the results
What's established: Testosterone influences desire. Declining testosterone contributes to reduced spontaneous desire. But testosterone is not the whole story — desire is far more complex than a single hormone.
Fluctuating Estrogen
Estrogen doesn't directly drive desire the way testosterone does — but its fluctuations create downstream effects that profoundly impact sexual interest and experience:
Vaginal dryness and atrophy → sex becomes uncomfortable or painful → desire decreases (who wants to do something that hurts?)
Mood instability → anxiety and depression reduce interest in sex
Sleep disruption → exhaustion eliminates the mental and physical space for desire
Changes in genital blood flow → reduced arousal and sensation
Estrogen's contribution to low libido is often indirect but significant.
Falling Progesterone and DHEA
Progesterone has a complex relationship with desire — it can have a mildly sedating effect, and its decline may alter the hormonal milieu that supports sexual receptivity
DHEA (dehydroepiandrosterone) is a precursor hormone that converts to both testosterone and estrogen. It declines with age and may contribute to changes in desire and arousal
The overall effect is a shifting hormonal ecosystem — not just one hormone falling, but the entire balance recalibrating
Physical Causes
Vaginal Dryness and Pain
This may be the single most impactful — and most treatable — physical cause of reduced sexual interest during perimenopause.
What's happening:
Declining estrogen thins the vaginal lining (vaginal atrophy)
Natural lubrication decreases — sometimes dramatically
Vaginal tissue loses elasticity and becomes more fragile
The vaginal pH changes, increasing susceptibility to irritation and infection
Sex becomes uncomfortable, painful, or anxiety-provoking
The vicious cycle: Pain during sex → anxiety about sex → avoidance of sex → less blood flow to genital tissue → further atrophy → more pain. This cycle can accelerate rapidly if not interrupted.
The critical point: This is one of the most effectively treatable causes of low libido. Vaginal estrogen, moisturizers, and lubricants can dramatically improve comfort — and when sex stops hurting, desire often begins to return.
Fatigue and Sleep Deprivation
Desire requires mental space and physical energy. During perimenopause, both are in short supply:
Night sweats disrupt sleep architecture
Insomnia leaves you running on empty
Fatigue makes your bed a place for sleep, not sex
By evening, you've used every drop of energy just getting through the day
Fatigue doesn't just reduce desire — it eliminates the context in which desire can emerge. You can't want something your body doesn't have the energy for.
Body Changes and Physical Discomfort
Weight redistribution may change how you feel in your body
Joint pain or muscle tension can make certain positions uncomfortable
Hot flashes can interrupt intimacy
Bloating and digestive discomfort can make you feel "unsexy" or physically closed off
These physical realities create barriers — not to love, but to the physical willingness to engage sexually.
Neurological and Psychological Causes
Brain Chemistry Changes
Desire isn't just a hormonal event — it's a neurological one. The brain networks involved in sexual motivation, reward processing, and emotional connection are all affected by perimenopausal hormonal shifts:
Serotonin fluctuations alter mood and can dampen libido (notably, SSRIs prescribed for mood can further suppress desire — see medication section)
Dopamine — the "motivation and reward" neurotransmitter — is influenced by estrogen. Changes may reduce the reward signal associated with sexual activity
Norepinephrine shifts affect arousal and attention
The prefrontal cortex (involved in decision-making and initiation) may be less activated toward sexual behavior when managing the cognitive load of perimenopause
In essence: your brain may be too busy managing hormonal chaos to prioritize sexual interest. This isn't a choice. It's neurobiology.
Anxiety, Depression, and Mood Shifts
Anxiety — particularly the physical, somatic anxiety common in perimenopause — creates a hypervigilant nervous system that's the opposite of the relaxed, open state required for desire
Depression — including the flat, low-motivation subtype common in perimenopause — directly suppresses libido
Mood volatility — the emotional roller coaster of perimenopause can leave you feeling too unstable to be vulnerable sexually
When your emotional world feels unsafe or unpredictable, sexual openness feels risky. Your brain protects you by shutting down the desire circuits.
Body Image and Identity
Perimenopause often coincides with visible changes in your body — weight, skin, hair, shape. In a culture that equates youth with desirability, these changes can profoundly affect how you see yourself as a sexual being:
"I don't feel attractive anymore"
"I don't recognize my body"
"I feel invisible"
"How can I be sexy when I don't feel like myself?"
These feelings are real and valid. They are also culturally constructed — which means they can be consciously deconstructed. But that work takes time, support, and a willingness to challenge the narratives you've absorbed.
Relational Causes
Libido doesn't exist in a vacuum. It exists in the context of your relationship — and midlife relationships carry their own complexity.
Communication Gaps
When desire changes and neither partner knows how to talk about it:
Silence builds → assumptions fill the gap → resentment grows
The partner with higher desire feels rejected
The partner with lower desire feels pressured or guilty
Both withdraw — emotionally and physically
Many couples describe a slow drift that began with unspoken libido changes and expanded into broader emotional distance.
Midlife Relationship Dynamics
Perimenopause often hits during a period of intense relational complexity:
Long-term relationship patterns may have calcified
Parenting demands may leave no space for couple time
Unresolved conflicts accumulate over decades
One or both partners may be experiencing their own midlife transition
Emotional intimacy may have eroded without anyone noticing
Low libido is sometimes a symptom of a relationship that needs attention — not just a hormonal event.
The Invisible Load
The mental load — planning, organizing, remembering, anticipating, managing everything for everyone — falls disproportionately on women. During perimenopause, this load becomes even heavier as you're simultaneously managing your own health crisis.
It's hard to desire sex when your brain is running a to-do list, worrying about an aging parent, managing a hormonal symptom, and processing the emotional needs of everyone around you.
Desire needs a quiet brain. The invisible load rarely allows one.
Medication-Related Causes
SSRIs/SNRIs and Libido
If you've been prescribed an antidepressant for perimenopause-related mood symptoms, it may be compounding your libido issue:
SSRIs (sertraline, fluoxetine, paroxetine, citalopram) are well-known to suppress desire, arousal, and orgasm
SNRIs (venlafaxine, duloxetine) have a similar but sometimes lesser effect
This side effect affects an estimated 40–65% of people taking these medications
The double bind: You may need mood support — but the treatment itself may worsen libido. This is worth discussing openly with your prescriber, because:
Some antidepressants have lower sexual side effects (bupropion/Wellbutrin is notable for this)
Dose adjustments or medication switches may help
Adding bupropion to an SSRI is sometimes used specifically to counteract sexual side effects
Hormonal Contraception Effects
Some women in perimenopause use hormonal contraception (pill, IUD, implant) — which can:
Increase sex hormone-binding globulin (SHBG), reducing free testosterone
Suppress ovarian hormone production
Create a hormonal environment that doesn't support spontaneous desire
If you're on hormonal contraception and experiencing significant libido changes, discuss alternatives with your provider.
Other Common Medications
Several commonly prescribed medications can affect libido:
Beta-blockers (for blood pressure or palpitations)
Antihistamines (including some used for sleep)
Gabapentin (sometimes prescribed for hot flashes)
Statins (for cholesterol — may affect hormone synthesis)
Opioids (suppress testosterone production)
A medication review with your provider — specifically asking about sexual side effects — can sometimes reveal modifiable factors.
What Science Says About Libido and Perimenopause
Testosterone — The Hormone Nobody Talks About in Women
What is established:
Women produce testosterone in the ovaries and adrenal glands
Testosterone declines gradually from the late 20s onward — by approximately 50% by midlife
Multiple studies (including the landmark New England Journal of Medicine testosterone patch trials) demonstrate that testosterone supplementation improves desire, arousal, and sexual satisfaction in postmenopausal women
The International Society for the Study of Women's Sexual Health (ISSWSH) endorses testosterone therapy for hypoactive sexual desire disorder (HSDD) in postmenopausal women
What is probable:
Testosterone plays a role in perimenopausal libido changes, not just postmenopausal
Individual variation in testosterone sensitivity may explain why some women experience dramatic libido changes while others don't
The brain's dopamine-reward system is testosterone-responsive — contributing to the "motivation" aspect of desire
What is still debated:
Optimal testosterone dosing for women (current guidelines recommend low physiological doses)
Long-term safety of testosterone supplementation in women (data beyond 2 years is limited)
Whether testosterone testing is clinically useful in women (poor correlation between levels and symptoms)
Availability and regulation (testosterone for women is not FDA-approved in the US, though it is prescribed off-label; it's available through some compounding pharmacies and is approved in Australia)
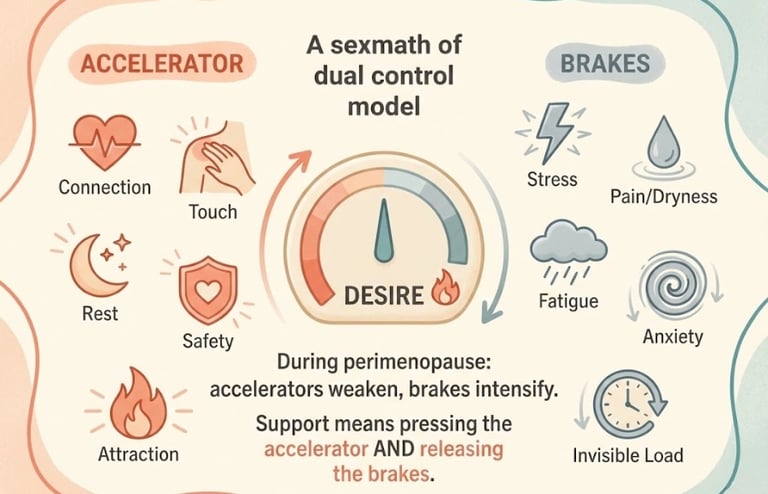
The Neuroscience of Desire — It's Not Just Hormones
Modern sexual health research has moved far beyond the "hormone = desire" equation. The dual control model of sexual response (developed by researchers at the Kinsey Institute) proposes that desire results from the balance between:
Sexual excitation (the "accelerator") — everything that activates desire: attraction, touch, fantasy, novelty, safety, connection
Sexual inhibition (the "brakes") — everything that suppresses desire: stress, pain, fatigue, anxiety, body image concerns, relationship tension, distraction
During perimenopause, the situation is often:
Reduced accelerator — less testosterone, less spontaneous desire, less genital sensitivity
Increased brakes — more fatigue, pain, anxiety, stress, body changes, hormonal chaos
The insight: Supporting libido during perimenopause isn't just about adding hormones (pressing the accelerator harder). It's equally — sometimes more — about removing the brakes: addressing pain, improving sleep, reducing anxiety, healing relationship dynamics, and creating the mental space for desire to emerge.
What's Established vs. What's Still Debated
Scientifically established:
Libido changes during perimenopause are common (40–55% of women)
Multiple hormonal, physical, psychological, and relational factors contribute
Vaginal estrogen effectively treats dryness and dyspareunia (pain during sex)
Testosterone supplementation improves desire in postmenopausal women (evidence strongest here)
SSRIs/SNRIs commonly cause sexual dysfunction
Responsive desire is a normal pattern of female sexuality
Probable (growing evidence):
Testosterone may benefit perimenopausal women with desire concerns (not just postmenopausal)
The estrogen-dopamine interaction plays a significant role in desire motivation
Mindfulness-based interventions can improve desire and arousal
Pelvic floor physiotherapy can enhance sexual function
Still debated:
Whether "low libido" should be considered a disorder or a normal variation during life transitions
Optimal treatment sequencing (hormonal vs. psychological vs. combined)
The role of flibanserin (Addyi) and bremelanotide (Vyleesi) in perimenopausal populations (currently only approved for premenopausal women)
Cultural vs. biological contributors to libido norms
What Actually Helps — Evidence-Based and Real-World Support
Start Here — The Things That Make the Biggest Difference First
Before exploring specific treatments, consider these foundational shifts — they address the most common barriers and often produce the most noticeable results:
Treat vaginal dryness and pain — if sex hurts, desire will not return until comfort does. This is step one.
Improve sleep — you cannot want sex when you're chronically exhausted. Addressing insomnia (through CBT-I, sleep hygiene, or hormonal support) creates the space for desire.
Review your medications — if you're on an SSRI, hormonal contraception, or another libido-suppressing medication, discuss alternatives with your provider.
Have the conversation — with your partner, and with yourself. Silence feeds shame. Communication opens possibilities.
Release the "should" — the pressure to want sex at a frequency that matches your past, your partner's desire, or cultural expectations is itself a brake on desire.
Addressing Vaginal Dryness and Discomfort
This is the most impactful, most evidence-based, and most immediately actionable step for many women.
Vaginal moisturizers (non-hormonal):
Used regularly (2–3 times per week), not just before sex
Help maintain tissue hydration and comfort
Hyaluronic acid-based options are well-tolerated
Examples: Hyalo GYN, Revaree, Replens
Lubricants (for sexual activity):
Water-based: easy to clean, compatible with condoms and toys; may need reapplication
Silicone-based: longer-lasting, more slippery; not compatible with silicone toys
Oil-based: long-lasting; not compatible with latex condoms
Avoid products with glycerin, parabens, chlorhexidine, or fragrances — these can irritate sensitive perimenopausal tissue
Look for ISO-certified, pH-balanced products when possible
Vaginal estrogen (prescription):
Available as cream (Estrace, Premarin), tablet (Vagifem), ring (Estring), or insert (Imvexxy)
Acts locally — very little systemic absorption
Restores vaginal tissue thickness, moisture, elasticity, and pH
Dramatically reduces pain during sex
Excellent safety profile — appropriate for most women, including many who cannot take systemic HRT
This is not "optional nice-to-have" — for women with GSM (Genitourinary Syndrome of Menopause), vaginal estrogen is first-line treatment per NAMS guidelines
The data: A Cochrane review confirmed that local vaginal estrogen is highly effective at relieving vaginal atrophy symptoms, including dyspareunia — and is significantly more effective than non-hormonal moisturizers alone.
Hormonal Options — HRT, Testosterone, and DHEA
Systemic Hormone Therapy (HRT)
Systemic estrogen (with progesterone if you have a uterus) can improve sleep, mood, vasomotor symptoms, and overall well-being — all of which indirectly support libido
HRT can improve genital blood flow and arousal in addition to its systemic effects
For some women, systemic HRT alone restores satisfactory sexual function
For others, it helps but isn't sufficient for desire specifically — testosterone may be the missing piece
Testosterone Therapy for Women
Available forms: Transdermal cream or gel (compounded), transdermal patch (not widely available)
Dose: Physiological female dose (approximately 1/10th of the male dose)
What it helps: Spontaneous desire, sexual thoughts, arousal, sensitivity, orgasm frequency and intensity
Evidence: The ADORE trial (Androgen supplementation for women's sexual function) and the New England Journal of Medicine testosterone patch trials demonstrated significant improvements in desire and satisfying sexual events
Current guidelines: The Global Consensus Position Statement on Testosterone Therapy for Women (2019) supports testosterone therapy for postmenopausal women with HSDD, used at physiological doses with monitoring
Availability: Not FDA-approved for women in the US. Available through compounding pharmacies and some menopause specialists. Approved in Australia. Available through some clinics in the UK
Monitoring: Lipid levels, liver function, and testosterone levels should be monitored. Watch for androgenic side effects (acne, facial hair growth) at higher doses
Important nuance: Testosterone therapy works best when other causes of low libido have been addressed — pain, mood, sleep, relationship dynamics. It's not a magic pill. But for the right woman, at the right dose, it can be genuinely transformative.
Vaginal DHEA (Intrarosa/Prasterone)
What it is: A vaginal insert containing DHEA, which is converted locally to both estrogen and testosterone
What it helps: Vaginal dryness, pain during sex, and may improve local arousal response
Advantage: Addresses both estrogenic and androgenic deficiency in vaginal tissue
Availability: FDA-approved (Intrarosa) in the US
Evidence: Clinical trials showed significant improvement in dyspareunia and vaginal dryness
Non-Hormonal Medical Options
Flibanserin (Addyi) and Bremelanotide (Vyleesi)
Both are FDA-approved for premenopausal women with HSDD (hypoactive sexual desire disorder)
Flibanserin: Daily oral tablet; acts on serotonin and dopamine pathways; modest efficacy; side effects include dizziness, nausea, fatigue; must avoid alcohol
Bremelanotide: Self-administered injection (before sexual activity); acts on melanocortin receptors; more targeted; side effects include nausea
Limitation: Neither is approved for perimenopausal or postmenopausal women. Evidence is limited in this population. Some clinicians prescribe off-label, but this should be a carefully considered decision
Bupropion (Wellbutrin)
An antidepressant that works on dopamine and norepinephrine — unlike SSRIs, it does not suppress libido and may actually enhance it
Sometimes used specifically as an adjunct to counteract SSRI-induced sexual dysfunction
Can also improve energy and motivation — both relevant in perimenopause
Worth discussing with your provider if you need mood support and are concerned about sexual side effects
Psychological and Relational Support
Sex Therapy and Couples Counseling
A sex therapist (certified by AASECT in the US or COSRT in the UK) can help you and your partner navigate desire discrepancy, communication, and intimacy
Couples counseling addresses the relational dynamics that may be contributing to low desire — resentment, communication patterns, emotional distance
These are not "last resort" options — they're often the most effective intervention, particularly when libido issues are relational as much as hormonal
Mindfulness-Based Interventions
Research from Dr. Lori Brotto (University of British Columbia) has demonstrated that mindfulness-based sex therapy can significantly improve sexual desire, arousal, and satisfaction in women — including those in midlife:
Mindfulness helps you stay present during sexual activity instead of being in your head
It reduces the anxiety and self-monitoring that suppress arousal
It helps reconnect with body sensations that may have become muted
This isn't abstract meditation. It's targeted, practical work — and the evidence for its effectiveness is growing.
Addressing Body Image
Working with a therapist who understands body image in midlife can be transformative
Challenging the narrative that only young, thin bodies are sexual bodies
Reconnecting with your body through movement, touch, and self-exploration — not just through the lens of how it looks
Lifestyle Shifts That Support Desire
These won't replace medical treatment when it's needed — but they create the conditions in which desire is more likely to emerge:
Sleep: Prioritize it ruthlessly. You cannot want sex while sleep-deprived. Address insomnia as a foundational step.
Exercise: Regular movement — especially strength training — supports testosterone, dopamine, body image, energy, and mood. All of these feed into desire.
Stress reduction: Your nervous system needs to feel safe for desire to activate. Whatever downregulates your stress response — breathwork, nature, boundaries, rest — supports libido indirectly.
Nutrition: Stable blood sugar, adequate protein, and anti-inflammatory eating support hormonal balance, energy, and mood — the infrastructure of desire.
Alcohol: Reducing or eliminating alcohol often improves desire. While alcohol may temporarily lower inhibition, it suppresses physical arousal, orgasm quality, and hormonal function.
Solo exploration: Reconnecting with your own body through masturbation — without pressure or goal — can help you rediscover what feels good now (which may be different from what felt good before).
🔎 Tools and Resources Worth Exploring
This article may contain affiliate links. We only recommend products we've researched and believe may be genuinely useful for women navigating perimenopause. Affiliate commissions help support this site at no extra cost to you.
1. "Come As You Are" by Dr. Emily Nagoski
Best for: Understanding the science of female desire — particularly the responsive desire model and the dual control (accelerator/brakes) framework
Why it helps here: This book is transformational for women who think their desire is broken. It reframes everything — from how desire works to why context matters more than hormones alone. Essential reading for any woman navigating libido changes
Strengths: Groundbreaking research presented accessibly, empowering, shame-dissolving, practical
Limitations: Not perimenopause-specific (covers female sexuality broadly)
2. Überlube (Silicone-Based Luxury Lubricant)
Best for: Women experiencing vaginal dryness who want a high-quality, long-lasting lubricant
Why it helps here: Silicone-based formula provides lasting lubrication without the tackiness of water-based options. Fragrance-free, glycerin-free, paraben-free. Designed to feel natural rather than clinical
Evidence context: Lubricants are recommended as first-line non-prescription support for vaginal dryness. Quality matters — cheap products often contain irritating ingredients
Strengths: Premium quality, body-safe ingredients, discreet packaging, long-lasting
Limitations: Not compatible with silicone toys; more expensive than basic options
3. Hyalo GYN (Hyaluronic Acid Vaginal Moisturizer)
Best for: Non-hormonal daily vaginal moisture support — used regularly, not just before sex
Why it helps here: Hyaluronic acid attracts and retains moisture in vaginal tissue. Used 2–3 times per week, it maintains tissue hydration and can significantly reduce discomfort. Hormone-free option for women who prefer or require non-hormonal approaches
Evidence context: Hyaluronic acid-based vaginal moisturizers have shown effectiveness comparable to low-dose vaginal estrogen in some studies for symptom relief
Strengths: Hormone-free, gentle, clinically studied, easy to use
Limitations: Less effective than vaginal estrogen for moderate-to-severe atrophy; requires consistent use
4. "The New Menopause" by Dr. Mary Claire Haver
Best for: Comprehensive understanding of perimenopause treatment options, including sexual health, HRT, and testosterone
Why it helps here: Covers the medical landscape of libido support including HRT, testosterone, and DHEA — helps you have an informed conversation with your provider
Strengths: Practical, evidence-based, empowering, addresses the full spectrum of treatment
Limitations: One clinical perspective — complement with individual guidance
5. Dame Products — Eva or Pom (Body-Safe Vibrators)
Best for: Women who want to reconnect with physical pleasure through solo or partnered exploration
Why it helps here: During perimenopause, genital sensitivity may decrease. Vibrators provide more intense, targeted stimulation that can help maintain neural pathways for arousal and orgasm. Medical literature supports vibrator use for improving arousal, lubrication, and orgasmic function in midlife women
Evidence context: A large survey published in the Journal of Sexual Medicine found vibrator use was associated with higher scores in desire, arousal, lubrication, and orgasm in women. Sex therapists frequently recommend vibrators as therapeutic tools, not just recreational ones
Strengths: Body-safe silicone, thoughtfully designed, discreet, rechargeable
Limitations: Personal preference varies; some women need time to overcome cultural discomfort with vibrators
YMYL disclosure: No product replaces medical consultation for significant sexual health concerns. Lubricants and moisturizers are supportive tools. Vibrators are associated with positive sexual health outcomes in research but are a personal choice. Hormone treatments require medical supervision. Individual results vary. Consult your healthcare provider for personalized guidance.
How to Talk About It — With Your Partner and Your Doctor
Starting the Conversation With a Partner
This is often the hardest part — harder than seeing a doctor, harder than trying a treatment. But silence is the greatest enemy of intimacy.
Framework for the conversation:
Choose the right moment. Not in bed. Not during an argument. Not after a rejection. Choose a calm, private, low-pressure moment.
Lead with connection, not complaint.
Instead of: "I never want sex anymore."
Try: "I want to talk about something that's been on my mind. I've noticed my desire has changed, and I want you to know it's not about you — it's something happening in my body."
Name what you know.
"I've learned that perimenopause can significantly affect libido — hormonally, physically, and emotionally. I'm trying to understand what's happening and what might help."
Express what you need.
"I need you to know this isn't rejection. I still want closeness. But I might need us to redefine what intimacy looks like right now."
Invite — don't assign.
"Would you be open to exploring this together? Maybe we could read something, or even talk to someone."
What your partner may need to hear most:
It's not about them
It's not a choice you're making
You still want connection — even if the form is changing
You want to work on this together, not suffer through it alone
What to Say to Your Doctor (And What to Ask For)
Many women avoid raising libido with their doctor — and many doctors avoid asking. Here's how to break that impasse:
Opening statement:
"I'd like to talk about my sexual health. My libido has changed significantly during perimenopause, and I'd like to explore what might be contributing and what options are available."
Specific questions to ask:
"Could vaginal dryness be contributing? Should we consider vaginal estrogen?"
"Would systemic HRT help with desire indirectly — through improving my sleep, mood, and overall symptoms?"
"What's your position on testosterone therapy for women? Is it something you'd consider prescribing or referring for?"
"I'm currently on [medication]. Could it be affecting my libido? Are there alternatives?"
"Can you refer me to a menopause specialist or sexual health specialist if this isn't your area of expertise?"
If your doctor dismisses you:
"I understand this is common, but it's causing me distress. I'd like to explore treatment options rather than accept it as inevitable."
Consider seeking a NAMS-certified menopause practitioner or a sexual medicine specialist (ISSWSH directory)
When to Seek a Specialist
Consider specialist referral when:
Your GP or gynecologist is unfamiliar with testosterone therapy for women
You have pain during sex that isn't resolving with lubricants alone
You want to explore the psychological and relational dimensions with professional support
You have complex medical history (cancer history, cardiovascular risk) that affects treatment options
You've tried first-line approaches and need more targeted intervention
Specialist options:
Menopause specialist (NAMS-certified)
Sexual medicine physician (ISSWSH certified)
Sex therapist (AASECT or COSRT certified)
Pelvic floor physiotherapist — if pain, tension, or muscle dysfunction is contributing
A New Definition of Intimacy
Redefining What "Good" Looks Like
One of the most liberating shifts a woman can make during perimenopause is releasing the definition of good sex that belonged to her 30-year-old self.
"Good" doesn't have to mean:
Frequent
Spontaneous
Penetrative
Ending in orgasm
Looking like it does in media
"Good" can mean:
Connected — feeling emotionally close before, during, and after
Comfortable — no pain, no pressure, no performance anxiety
Present — being in your body, not in your head
Pleasurable — in whatever form that takes today
Chosen — engaging because you want to, not because you should
Pleasure Beyond Penetration
If penetrative sex has become uncomfortable, less satisfying, or simply less interesting — there is an entire universe of intimacy that doesn't require it:
Extended kissing and touch
Mutual massage
Oral intimacy
Use of vibrators or other aids
Sensual baths or showers together
"Outercourse" — genital stimulation without penetration
Intimate conversation and emotional vulnerability
Physical closeness without sexual expectations — holding, cuddling, skin contact
These are not consolation prizes. They are legitimate, complete forms of sexual and intimate expression. For many couples in midlife, expanding the definition of intimacy actually leads to greater satisfaction than trying to replicate the sex life of 15 years ago.
The Permission to Evolve
Your sexuality is not fixed. It was never supposed to be.
At 20, desire was driven by novelty, hormones, and discovery. At 30, it may have been shaped by partnership and deepening connection. At 45 or 50, it's being reshaped again — by hormonal changes, life experience, and a more complex understanding of what you need.
This evolution is not a decline. It's a transformation.
Some women find that perimenopause ultimately leads them to a more authentic, more intentional, and more satisfying sexual life — because it forced them to examine what they actually want, communicate honestly, and stop performing.
That doesn't mean the transition is easy. It isn't. But there is something on the other side that can be genuinely good — if you give yourself permission to let it be different from what came before.
You're Not Broken — Your Desire Is Changing Shape
If you've read this far, you probably came here carrying some combination of confusion, frustration, guilt, and grief. You may have been blaming yourself. You may have been blaming your partner. You may have been hoping for a simple fix.
Here's what we hope you're taking away instead:
Your libido change is real. It has biological, physical, neurological, and relational causes — and none of them are your fault.
You're not alone. The majority of women experience some change in desire during perimenopause. The silence around it doesn't reflect its rarity — it reflects our cultural discomfort with honest conversations about female sexuality.
There is support available. From vaginal estrogen to testosterone therapy, from lubricants to sex therapy, from mindfulness to simple communication — there are options. Not all of them work for every woman. But most women can find a combination that helps.
Your desire is not gone. It's changing shape. It may need different conditions to emerge. It may look different from what you're used to. It may require you to redefine intimacy, explore new pathways to pleasure, and let go of expectations that no longer serve you.
That's not a loss. That's growth.
And you deserve support through every bit of it.
FAQ — Low Libido During Perimenopause
Q: Is low libido normal during perimenopause?
A: Yes. An estimated 40–55% of women experience reduced sexual desire during the menopausal transition. It's caused by declining testosterone, fluctuating estrogen, physical changes, mood shifts, and fatigue. It's common, biological, and not a personal failure.
Q: Does HRT help with low libido in perimenopause?
A: HRT can help indirectly by improving sleep, mood, energy, and vaginal comfort — all of which support desire. For desire specifically, testosterone therapy may be more directly effective. Discuss both options with a menopause-informed provider.
Q: Can testosterone therapy help women's libido?
A: Yes. Research shows testosterone therapy at physiological doses can improve desire, arousal, and sexual satisfaction in women. It's endorsed by the ISSWSH for postmenopausal HSDD. Availability varies — discuss with a menopause specialist.
Q: Why does vaginal dryness affect libido?
A: When sex becomes painful due to vaginal dryness and thinning tissue, your brain creates a negative association — pain replaces pleasure, and desire naturally decreases. Treating dryness with vaginal estrogen, moisturizers, or lubricants is often the most impactful first step.
Q: Can antidepressants cause low libido during perimenopause?
A: Yes. SSRIs and SNRIs — commonly prescribed for perimenopausal mood symptoms — suppress desire, arousal, and orgasm in an estimated 40–65% of users. Bupropion is an alternative with lower sexual side effects. Discuss options with your prescriber.
Q: What is responsive desire?
A: Responsive desire is desire that emerges in response to stimulation, connection, and context — rather than appearing spontaneously. Approximately 70% of women experience primarily responsive desire. During perimenopause, the shift from spontaneous to responsive desire is very common and not a dysfunction.
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References


Perimenopause Compass
Contact
Newsletter
hello@perimenopausecompass.com
© 2026 All rights reserved.