Irregular Periods in Perimenopause: What's Normal?
Irregular periods in perimenopause can be confusing and alarming. Learn what's normal, what's not, when to see your doctor, and why your cycle is changing — explained clearly and honestly.
LIFESTYLE
Perimenopause Compass
2/25/202623 min read
Your period used to be predictable. Maybe not to the hour, but you knew — roughly when it would come, how long it would last, how heavy it would be. It was background noise. Unremarkable. Reliable.
And then it wasn't.
Maybe it came early. Then late. Then heavy — heavier than you've ever seen. Then it vanished for two months and you thought it was over. Then it came back, lighter this time, lasting nine days instead of five. Then you had spotting mid-cycle for no reason. Then nothing for six weeks.
And through all of it, one question kept echoing: is this normal?
If you're between 40 and 55 and your period has started behaving in ways you don't recognize, the answer is almost certainly yes — what you're experiencing is within the wide range of normal for perimenopause.
But "normal" is a big word. It covers everything from slightly shorter cycles to flooding through a super tampon in an hour. And the line between "normal perimenopausal change" and "something that needs medical attention" isn't always obvious.
This article draws that line clearly. You'll learn every way periods can change during perimenopause, exactly why it happens, when it's normal, and when you need to see your doctor. No vague reassurances. No unnecessary alarm. Just the honest, detailed information your body deserves.
The Question Behind Every Skipped, Heavy, or Unpredictable Period
Why Period Changes Create So Much Anxiety
Of all perimenopause symptoms, menstrual changes generate a unique kind of anxiety — because your period has always been a health signal.
From puberty, you were taught (implicitly or explicitly) that your period reflects your health:
Regular = healthy
Irregular = something's wrong
Heavy = investigate
Missing = pregnant or problem
These deeply ingrained associations don't disappear at 45. So when your period starts acting unpredictably, your brain defaults to alarm mode — even when the changes are entirely expected for your stage of life.
The anxiety is compounded by:
Fear of serious conditions — "What if this heavy bleeding is cancer?"
Pregnancy uncertainty — "Could I be pregnant at 46?"
Loss of predictability — "I used to know my body. Now I don't."
Medical dismissal — "My doctor said 'that's just perimenopause' — but how do I know it's JUST perimenopause?"
Social disruption — flooding, unpredictable timing, and prolonged bleeding affect work, travel, intimacy, and confidence
Your anxiety is not irrational. It's a reasonable response to significant bodily change combined with inadequate information. This article aims to fill that gap.
What This Guide Covers
This guide will give you:
The biology — why your periods change, in plain language
The full spectrum — every type of period change that falls within normal perimenopause
Clear red flags — exactly when to seek medical attention
Real women's experiences — so you know you're not alone
Practical management — what helps, from tracking to treatment
Contraception guidance — because yes, you can still get pregnant
This article is for educational purposes and does not replace medical advice. If you're experiencing menstrual changes that concern you, consult a healthcare provider.
Why Your Periods Change During Perimenopause
The Hormonal Mechanics — Simply Explained
Your menstrual cycle is orchestrated by a feedback loop between your brain and your ovaries. Here's the simplified version:
Your pituitary gland (in the brain) sends FSH (follicle-stimulating hormone) to your ovaries
FSH stimulates a follicle to develop and produce estrogen
Rising estrogen triggers a surge of LH (luteinizing hormone) → ovulation occurs
After ovulation, the empty follicle produces progesterone
If pregnancy doesn't occur, progesterone and estrogen drop → your uterine lining sheds → period
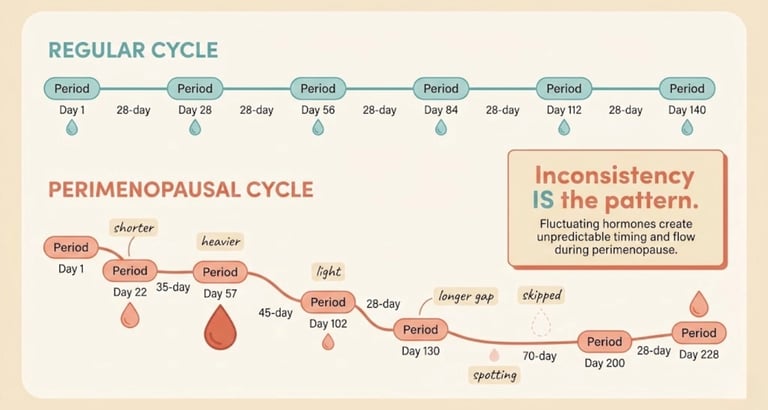
This cycle repeats roughly every 28 days (though 21–35 days is considered normal).
During perimenopause, every step in this process becomes less reliable:
Your ovaries respond less consistently to FSH → your brain produces more FSH to try harder → sometimes this overstimulates estrogen production (paradoxically)
Ovulation becomes unpredictable — sometimes it happens, sometimes it doesn't, sometimes it's delayed
Without ovulation, progesterone isn't produced → your uterine lining keeps growing under estrogen's influence without the normal "reset"
The lining eventually sheds anyway — but irregularly, incompletely, or all at once → explaining the heavy, prolonged, or unpredictable bleeding
The bottom line: Your period changes because the hormonal conversation between your brain and ovaries is breaking down. It's not a malfunction — it's the natural winding down of reproductive function. But the process is messy, gradual, and nonlinear.
Ovulation Becomes the Wild Card
Ovulation is the pivotal event in your cycle. When it happens, your cycle follows a recognizable pattern. When it doesn't, everything shifts.
In perimenopause, ovulation becomes a wild card:


In any given month during perimenopause, you don't know which of these scenarios your body will choose. This is why periods become so unpredictable — each cycle may follow a different ovulatory pattern.
Why the Changes Are Gradual (Then Suddenly Not)
Most women describe perimenopausal period changes as following a pattern of slow drift → sudden disruption:
Years 1–3: Subtle changes — slightly shorter cycles, marginally heavier flow, PMS intensifying. Easy to dismiss.
Years 3–5: More noticeable — cycles varying by a week or more, occasional skipped period, episodes of heavy bleeding.
Years 5+: Unmistakable — large gaps between periods (60, 90, 120+ days), unpredictable flooding, or a confusing mix of spotting and nothing.
This progression maps onto the STRAW+10 stages of reproductive aging (more on this in the science section). Understanding that the changes tend to escalate helps normalize the experience — and helps you recognize that each shift is a step forward in the transition, not a sign that something has gone wrong.
What's Normal — The Full Spectrum of Perimenopausal Period Changes
This is the section you probably came here for. Let's be comprehensive.
Important framing: "Normal" in perimenopause covers an extraordinarily wide range. What would be considered abnormal in a premenopausal woman — a cycle of 22 days, or 45 days, or a period lasting 8 days — may be completely normal during the transition.
The key question isn't "is this exactly like my period used to be?" — it's "is this within the expected range for a body going through perimenopause?"
Here's every major change, what causes it, and when it crosses from expected to concerning.
Shorter Cycles (Less Than 25 Days)
What it looks like:
Your cycle shrinks from 28–30 days to 24, 23, or even 21 days
You feel like you're "always getting your period"
You may be buying tampons and pads more frequently than ever
Why it happens:
In early perimenopause, the follicular phase (the first half of your cycle) often shortens. Your ovaries are working harder and faster, sometimes producing follicles — and therefore estrogen — more quickly.
FSH is elevated, accelerating the process
The luteal phase (after ovulation) may also shorten slightly
Is it normal? Yes. Shortened cycles are one of the earliest and most common perimenopausal changes. They may persist for months or years before cycles begin to lengthen.
When to note it: If cycles are consistently shorter than 21 days, or if the frequency is causing quality-of-life issues (constantly menstruating), discuss with your provider.
Longer Cycles (35+ Days, Then 60+ Days)
What it looks like:
Your cycle gradually stretches — 32 days, then 38, then 45
Eventually, gaps of 60, 90, or even 120+ days may occur
You stop being able to predict when your next period will come
Why it happens:
Ovulation is becoming more infrequent — sometimes your body tries to ovulate, fails, and tries again, delaying the cycle
Without ovulation, there's no progesterone-driven shedding — the lining sits and waits until estrogen drops enough, or builds until it outgrows its blood supply and sheds on its own
The brain-ovary feedback loop is becoming less responsive
Is it normal? Yes. Progressively longer and more irregular cycles are the defining feature of mid-to-late perimenopause. Per STRAW+10 criteria, a gap of ≥60 days between periods signals you've moved into late menopausal transition.
When to note it: Longer cycles themselves aren't concerning — but if a period returns after a long gap and is extremely heavy, it's worth monitoring and potentially investigating (see the section on heavy bleeding below).
Skipped Periods — Then They Come Back
What it looks like:
You miss a period entirely — one month, two months, three months
You start wondering if menopause has arrived
Then your period returns — sometimes normally, sometimes with a vengeance
Why it happens:
Anovulatory months become more frequent — no ovulation means no hormonal trigger for shedding
The lining may quietly reabsorb, or sit dormant until a later hormonal shift triggers shedding
One anovulatory cycle may be followed by a normal ovulatory cycle — hence the "return"
Is it normal? Completely. The false finish — thinking your periods are over, only to have them return — is one of the most commonly reported perimenopausal experiences. Remember: menopause is only confirmed after 12 consecutive months without a period. Until then, return of bleeding is expected.
When to note it: If bleeding returns after 12+ months of absence, this is technically postmenopausal bleeding and should be evaluated by your doctor to rule out other causes (see red flags section).
Heavier Periods and Flooding
What it looks like:
Periods that are noticeably heavier than your historical norm
Flooding — sudden, heavy gushes of blood that overwhelm your protection
Soaking through a pad or tampon in less than 2 hours
Passing large blood clots (quarter-sized or larger)
Needing to use double protection (pad + tampon, or period underwear + pad)
Having to get up at night to change protection
Periods that last 7, 8, 9+ days
Feeling physically drained or lightheaded during heavy periods
Why it happens:
Anovulatory cycles allow the uterine lining to build up under unopposed estrogen — without progesterone to stabilize and limit growth. When the lining finally sheds, there's more of it, and the shedding is less organized
Estrogen spikes — paradoxically, estrogen can surge to very high levels during perimenopause, stimulating significant endometrial growth
The uterine lining may not shed evenly, leading to prolonged or stop-start bleeding
Fibroids (noncancerous uterine growths) are common in women over 40 and can worsen with estrogen fluctuations, contributing to heavier bleeding
Adenomyosis (endometrial tissue growing into the uterine muscle wall) can also be a factor
Is it normal? Heavier periods are common in perimenopause — particularly in the mid-transition (ages 44–50). However, there is a line between "heavier than usual" and "medically concerning heavy bleeding" (menorrhagia).
Where's the line?
You should see your doctor if:
You're soaking through a pad or tampon every hour for 2+ consecutive hours
You're consistently passing clots larger than a quarter/£1 coin
Heavy bleeding lasts more than 7 days
You're experiencing symptoms of anemia: persistent fatigue, dizziness, shortness of breath, pale skin, heart pounding
Heavy bleeding is significantly disrupting your daily life — missing work, canceling plans, afraid to leave the house
This is important: Heavy perimenopausal bleeding is usually caused by hormonal changes. But it can also be caused by fibroids, polyps, adenomyosis, endometrial hyperplasia, or — rarely — endometrial cancer. Investigation doesn't mean something terrible is happening. It means being thorough. And being thorough is how serious conditions get caught early and treated effectively.
Lighter Periods and Spotting
What it looks like:
Periods that are barely there — light spotting for a day or two
Needing only a panty liner instead of your usual protection
Brownish or pinkish discharge rather than red flow
Spotting between periods (intermenstrual bleeding)
Spotting that replaces a full period
Why it happens:
Anovulatory cycles with minimal lining buildup
Declining estrogen reducing endometrial thickness
Incomplete shedding — only part of the lining comes away
Hormonal fluctuations creating mid-cycle spotting
Is it normal? Yes. Lighter periods and spotting are common, especially in late perimenopause as estrogen levels trend consistently lower. For many women, periods gradually become lighter and less frequent before stopping altogether.
When to note it: Persistent intermenstrual spotting (bleeding between periods) or postcoital bleeding (bleeding after sex) should be evaluated — not because it's necessarily serious, but because these patterns can sometimes indicate cervical changes, polyps, or other conditions that benefit from investigation.
Longer or Shorter Bleeding Duration
What it looks like:
Periods that last 8, 9, or 10+ days instead of your usual 4–5
Or the opposite — periods that are over in 2 days when they used to last 5
Duration varying from cycle to cycle — 3 days one month, 9 days the next
Why it happens:
Longer bleeding: Anovulatory cycles produce an unstable lining that doesn't shed efficiently. Instead of a clean, organized shedding (which produces a typical 4–5 day period), the lining comes away in patches over many days.
Shorter bleeding: When there's less lining buildup (due to lower estrogen or a cycle following close behind another), the shedding is quick and light.
Variable duration: Different hormonal scenarios each month produce different lining characteristics — hence the unpredictability.
Is it normal? Yes, within limits. Bleeding that consistently exceeds 8–10 days or that is both prolonged and heavy warrants medical evaluation.
Changes in Clotting
What it looks like:
Larger blood clots than you've seen before
Clots that are dark red, almost liver-colored
Clots accompanying heavy flow
Why it happens:
When bleeding is heavy and fast, your body's natural anticoagulant system (which normally keeps menstrual blood liquid) can be overwhelmed — resulting in clot formation
A thicker uterine lining sheds in larger pieces
This is a mechanical response, not a clotting disorder
Is it normal? Small to moderate clots during heavy perimenopausal periods are common. Clots that are consistently larger than a quarter/£1 coin should be discussed with your doctor — not because they're necessarily dangerous, but because they indicate very heavy bleeding that may need management.
Unpredictable Timing — No Pattern at All
What it looks like:
You genuinely cannot predict when your next period will come
Your tracking app has given up trying to forecast
Periods are 22 days apart, then 45, then 30, then 70
You carry protection everywhere "just in case"
Why it happens:
Each cycle is governed by a different hormonal scenario — whether and when you ovulate, how much estrogen your ovaries produce, how the lining responds
There's no "master pattern" anymore — each month is its own event
Is it normal? Extremely. This is textbook mid-to-late perimenopause. Per STRAW+10 criteria, cycles that vary by ≥7 days from your personal baseline signal early menopausal transition. Increasing variability and unpredictability are expected to continue until periods stop entirely.
Your Period Looks Different in Every Way
Some women experience all of the above — sometimes within a few months of each other. A short, light period followed by a 10-day flood. A skipped month followed by two periods in three weeks. An entirely new type of cramping, or no cramps at all when you used to have them.
Is it normal? Yes. The only consistent thing about perimenopausal periods is their inconsistency. Your body is navigating a hormonal transition that doesn't follow a script — and your menstrual cycle reflects that reality month by month.
What Women Actually Experience — Period Stories Nobody Tells
"I Went Through a Super Tampon in an Hour"
"At 47, I had the heaviest period of my life. I was at work. I could feel the gush — and by the time I got to the bathroom, my chair had a stain. I changed a super tampon and within 45 minutes, I'd soaked through it. I sat on the toilet for 20 minutes passing clots the size of golf balls. I was shaking. I called my husband to pick me up because I was afraid to stand on the train. My doctor later confirmed it was a classic anovulatory bleed — months of estrogen building up the lining, then everything coming away at once. I wasn't dying. But nobody had warned me this could happen."
"My Period Disappeared for Three Months — Then Came Back With Vengeance"
"At 49, I went 90 days without a period. I was cautiously celebrating. Then it arrived — and it lasted 12 days. Heavy for the first four, then spotting, then heavy again, then nothing for a day, then spotting again. It was like my uterus couldn't make up its mind. My GP ordered an ultrasound to check my lining thickness and rule out polyps. Everything was clear. It was 'just' perimenopause. I've never been so relieved — and so exhausted — by a diagnosis."
"I Have Two Periods a Month Now"
"At 43, my cycles shortened to 21 days. I was having two periods a month. FOURTEEN days per month of bleeding. I was exhausted, anemic, and my ferritin had dropped to 8 (it should be above 30). Nobody connected the dots until I insisted on iron studies. The heavy, frequent periods were causing iron deficiency — and the iron deficiency was making the fatigue and brain fog exponentially worse. Once I started iron supplementation and my doctor put me on a hormonal IUD to manage the bleeding, everything changed."
"I Don't Know What Day My Period Will Come Anymore"
"I used to be 28 days like clockwork. For 25 years. Now? I haven't had a predictable cycle in 18 months. My period shows up when it wants — 19 days, 40 days, 33 days. I've ruined underwear, bed sheets, a car seat. I carry a 'period emergency kit' in my bag at all times. I know intellectually that this is perimenopause. But emotionally, it feels like losing control of my own body. And nobody in my life — not my friends, not my mother, not my doctor — told me this was coming."
What's NOT Normal — When to See Your Doctor
This is the section that matters most for your safety. While the vast majority of perimenopausal period changes are hormonal and benign, some patterns require medical evaluation to rule out conditions that need treatment.
The Red Flags You Shouldn't Ignore
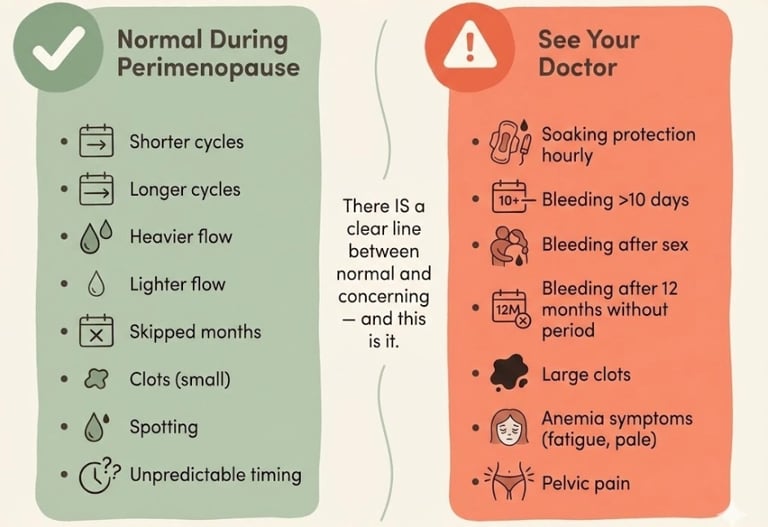
See your doctor promptly if you experience any of the following:
🚩 Soaking through a pad or tampon every hour for 2 or more consecutive hours
🚩 Bleeding that lasts more than 10 days — especially if heavy throughout
🚩 Bleeding after sex (postcoital bleeding) — even spotting
🚩 Bleeding after 12+ months without a period (postmenopausal bleeding — always investigate)
🚩 Persistent intermenstrual bleeding — bleeding between periods that recurs over multiple cycles
🚩 Symptoms of anemia — persistent fatigue, dizziness, shortness of breath, heart pounding, pale skin, difficulty concentrating
🚩 Pelvic pain that is new, persistent, or worsening
🚩 Significant change in vaginal discharge — especially if bloody or foul-smelling
🚩 Periods becoming dramatically heavier over a short period of time — a sudden escalation rather than a gradual change
Heavy Bleeding — How to Tell If It's Too Heavy
"Heavy" is subjective — what feels heavy to one woman may be moderate to another. Here's a more objective framework:
Your bleeding may be medically significant (menorrhagia) if:
If 2 or more of these apply, an evaluation is warranted — not to alarm you, but to ensure appropriate management.
What your doctor will likely do:
Blood count and iron/ferritin levels — to check for anemia
Pelvic ultrasound — to assess endometrial thickness, check for fibroids or polyps
Endometrial biopsy — if the lining is significantly thickened or if you have risk factors for endometrial hyperplasia
Thyroid function — hypothyroidism can cause heavy periods
Coagulation screen — if there's a family history of bleeding disorders
Bleeding After Sex
Postcoital bleeding (bleeding after sexual intercourse) during perimenopause can be caused by:
Vaginal atrophy — thinning vaginal tissue that is easily irritated (most common cause)
Cervical ectropion — a benign condition where cells from inside the cervix are visible on the outside
Cervical polyps — usually benign growths
Cervical changes — including, rarely, precancerous or cancerous changes
Action: Postcoital bleeding should be evaluated — typically with a cervical examination and ensuring your cervical screening (Pap smear/HPV test) is up to date. Most causes are benign, but investigation is important.
Bleeding After 12 Months Without a Period
This is the one that requires the most emphasis:
If you have not had a period for 12 or more consecutive months, and then you experience vaginal bleeding — see your doctor.
This is classified as postmenopausal bleeding and should be investigated. Possible causes include:
Vaginal atrophy (most common and most benign)
Endometrial polyps
Endometrial hyperplasia (thickening of the uterine lining)
Endometrial cancer (uncommon, but this is the primary reason postmenopausal bleeding is always investigated)
HRT-related bleeding (if you've recently started or changed hormone therapy)
Investigation typically includes a pelvic ultrasound to measure endometrial thickness and potentially an endometrial biopsy or hysteroscopy.
The reassuring truth: The majority of postmenopausal bleeding is caused by benign conditions. But investigation is essential because early detection of the serious causes dramatically improves outcomes.
Other Warning Signs
See your doctor if:
You have a family history of endometrial or ovarian cancer and are experiencing new bleeding changes
You have obesity, diabetes, or polycystic ovary syndrome (PCOS) — these increase the risk of endometrial hyperplasia
You are taking tamoxifen (for breast cancer) — which increases endometrial cancer risk
You experience unexplained weight loss alongside bleeding changes
Conditions to Rule Out
The message: Investigation isn't a reason to panic. It's a reason to feel empowered. You're not being hysterical for seeking an evaluation. You're being responsible. And most of the time, the result is reassurance — plus, when it's needed, a treatable condition caught early.
What Science Says About Perimenopausal Periods
The STRAW+10 Menstrual Criteria — Where You Are in the Timeline
The Stages of Reproductive Aging Workshop (STRAW+10) uses menstrual cycle changes as the primary marker for staging the menopausal transition. Here's how your period patterns map to the stages:
How to use this:
If your cycles are just starting to vary (some shorter, some longer, more than 7 days different from your usual), you're likely in Stage -2 (early transition)
If you've had gaps of 60+ days, you've likely entered Stage -1 (late transition)
If it's been 12 months since your last period, you've reached menopause
Your menstrual pattern is the most reliable, accessible marker of where you are in the transition — more reliable than any blood test during perimenopause.
What the SWAN Study Tells Us About Bleeding Patterns
The Study of Women's Health Across the Nation (SWAN) — the largest longitudinal study of the menopausal transition — has provided crucial data on menstrual changes:
Shorter cycles are typically the first change — occurring in the early forties for many women
Episodes of heavy bleeding increase during mid-transition — one SWAN analysis found that women in late perimenopause had a threefold increase in heavy bleeding days compared to premenopausal women
Very long cycles (60+ days) typically appear 1–3 years before the final menstrual period
Bleeding episodes lasting 10+ days occur in approximately 25–30% of women during the transition
Racial and ethnic differences exist: Black women tend to experience more heavy bleeding days during perimenopause compared to white and Asian women
What this data tells you: Heavy, prolonged, and unpredictable bleeding during perimenopause is not rare — it's experienced by a significant minority (and arguably a majority, if you count all variations of "heavier than before"). You're not an outlier. You're in the norm.
Established vs. Probable vs. Still Being Studied
Scientifically established:
Menstrual irregularity is the hallmark of perimenopause
Changes progress from subtle (shorter cycles) to obvious (skipped periods, heavy bleeding) over years
Anovulatory cycles are the primary driver of heavy, irregular bleeding
STRAW+10 menstrual criteria are the international standard for staging
Most abnormal bleeding in perimenopause is hormonal — but structural causes should be ruled out
Probable (growing evidence):
The intensity of bleeding changes may correlate with the severity of vasomotor symptoms
Gut microbiome health (estrobolome) influences estrogen recycling, which may affect lining growth
Inflammatory markers contribute to the heaviness and pain of perimenopausal periods
Lifestyle factors (exercise, nutrition, alcohol) may modulate bleeding severity
Still debated:
Optimal threshold for when to biopsy vs. observe in perimenopausal heavy bleeding
Whether earlier intervention (e.g., hormonal IUD placement in early perimenopause) reduces bleeding burden over the transition
The role of endometrial thickness measurement as a screening tool during perimenopause (it's well-established postmenopause, less clear during the transition)

How to Track Your Changing Cycle
What to Record and Why It Matters
Tracking your cycle during perimenopause serves three critical purposes:
It reveals your STRAW stage — showing you where you are in the transition based on cycle length patterns
It documents change over time — making it easier to distinguish gradual hormonal change from sudden concerning shifts
It gives your doctor actionable data — a 3–6 month tracking log is worth more than a single blood test
The Tracking Method That Helps Your Doctor Help You
Record the following for each cycle:
After 3–6 months, this data creates a clinical picture that helps your provider:
Determine if investigation is needed
Stage your transition
Choose appropriate management
Monitor treatment effectiveness
🔎 Tools and Resources for Cycle Tracking
This article may contain affiliate links. We only recommend products we've researched and believe may be genuinely useful for women in perimenopause. Affiliate commissions help support this site at no extra cost to you.
1. Balance App (by Dr. Louise Newson)
Best for: Free, menopause-specific tracking that generates shareable health reports
Why it helps here: Tracks cycle patterns alongside other perimenopause symptoms, creating a comprehensive picture. The health report feature is designed for medical consultations
Strengths: Free, medically informed, connects bleeding to overall symptom pattern
Limitations: UK-developed; some content less US-relevant
2. Oura Ring (Gen 3)
Best for: Objective temperature and biometric data that correlates with ovulation and cycle phase
Why it helps here: Tracks basal body temperature trends — which can help identify whether you're ovulating (temperature rise after ovulation) and predict cycle changes. Useful for understanding the ovulation wild card
Strengths: Objective data, identifies ovulation patterns, longitudinal tracking
Limitations: $299+ investment, subscription required, complementary to (not replacement for) symptom tracking
3. Period Underwear (Modibodi or Knix)
Best for: Managing unpredictable bleeding with confidence — especially when you don't know when your period will arrive
Why it helps here: During perimenopause, period timing is unpredictable. Period underwear provides backup protection you can wear daily without discomfort. Also useful for heavy days as a secondary layer
Evidence context: Not a medical tool, but a practical support that significantly reduces the anxiety of unpredictable bleeding — which is one of the most commonly reported quality-of-life impacts of perimenopausal periods
Strengths: Reusable, comfortable, reduces waste and cost, available in heavy-flow options
Limitations: Not sufficient alone for very heavy days (flooding); requires washing
4. Iron Bisglycinate Supplement (Gentle Iron)
Best for: Women experiencing heavy periods who may be iron-depleted
Why it helps here: Heavy perimenopausal bleeding is a leading cause of iron deficiency in women over 40. Symptoms of iron deficiency — fatigue, brain fog, breathlessness, palpitations, poor concentration — overlap with and amplify perimenopause symptoms. Iron bisglycinate is the gentlest, best-absorbed form
Evidence level: Iron replacement for confirmed deficiency is well-established medicine. Test before supplementing (serum ferritin is the most sensitive marker)
Important: Do NOT supplement iron without testing first — excess iron can be harmful. Ask your doctor for ferritin, serum iron, and transferrin saturation levels. Target ferritin: above 30 ng/mL at minimum; above 50 ng/mL is optimal for symptom resolution
Look for: Bisglycinate form (gentle on stomach), third-party tested
YMYL disclosure: Iron supplementation should only be started after blood testing confirms deficiency. Excess iron can be harmful. Period underwear and tracking tools are practical aids, not medical treatments. Always consult your healthcare provider for personalized guidance on managing heavy bleeding.
Managing Irregular Periods — What Actually Helps
When No Treatment Is Needed
Not all perimenopausal period changes require treatment. If your periods are:
Mildly irregular but not significantly heavier
Not causing anemia
Not significantly disrupting your quality of life
Within the expected range for your transition stage
Then monitoring and tracking may be all that's needed. Understanding that the changes are normal — and having the framework to recognize when they cross a line — is itself a form of management.
Managing Heavy Bleeding — Medical Options
For women whose bleeding is significantly heavy, prolonged, or causing anemia, several effective medical options exist:
Hormonal IUD (Mirena/Levonorgestrel IUD):
Releases a small amount of progesterone directly into the uterus
Dramatically reduces menstrual bleeding — up to 90% reduction within 6 months
Provides contraception simultaneously
Provides the progesterone component if you later start estrogen-based HRT
Effective for 5–8 years (depending on device)
First-line recommendation by NICE and ACOG for heavy menstrual bleeding
Side effects: irregular spotting initially (usually settles), some women experience hormonal effects
Tranexamic acid (Lysteda):
Non-hormonal medication taken during heavy bleeding days
Works by stabilizing blood clots, reducing bleeding by approximately 30–50%
Taken only during heavy days — not continuously
Available by prescription (UK and US)
Can be used alongside other treatments
NSAIDs (Ibuprofen, Naproxen):
Reduce both bleeding volume (by approximately 20–30%) and cramping
Work by reducing prostaglandin production
Available over the counter
Most effective when taken at the first sign of bleeding, before it becomes heavy
Hormonal Options — HRT, Progesterone, and Hormonal IUDs
Cyclical progesterone:
Taking progesterone (usually micronized progesterone/Prometrium) for 12–14 days per cycle can regulate shedding and reduce heavy, unpredictable bleeding
This mimics the natural progesterone phase that anovulatory cycles lack
Can also improve sleep and reduce anxiety (bonus perimenopausal benefits)
Requires a prescription and should be discussed with your provider
Combined HRT (estrogen + progesterone):
For women in later perimenopause who need symptom management beyond just bleeding
Can regulate cycles while also addressing hot flashes, sleep, mood
The progesterone component protects the endometrium
Hormonal IUD + estrogen:
Many menopause specialists recommend a Mirena IUD (for endometrial protection and bleeding control) plus transdermal estrogen (patch or gel) — this combination addresses both bleeding and systemic symptoms
Increasingly recognized as one of the most effective and well-tolerated approaches for perimenopausal women
Non-Hormonal Options
Endometrial ablation:
A procedure that destroys the uterine lining, dramatically reducing or eliminating bleeding
Effective for women who are certain they don't want future pregnancies
Not suitable for all women (depends on uterine anatomy and presence of fibroids)
Does not provide contraception — you can still ovulate and potentially conceive (with serious risks to any pregnancy)
Fibroid management:
If fibroids are contributing to heavy bleeding, options include medication (GnRH agonists), uterine artery embolization, myomectomy (fibroid removal), or — for severe cases — hysterectomy
Management depends on fibroid size, location, and your symptoms
Hysterectomy:
Definitive solution for heavy bleeding — removal of the uterus
Major surgery with recovery time
Considered when other treatments have failed or aren't appropriate
Ovaries may be preserved (continuing natural hormonal function) or removed (causing immediate surgical menopause)
Should be a carefully considered decision, not a first-line response
Iron and Nutritional Support
Heavy perimenopausal bleeding is the leading cause of iron deficiency in women over 40. This is critically important because iron deficiency symptoms — fatigue, brain fog, breathlessness, difficulty concentrating, palpitations, dizziness — overlap with and worsen perimenopause symptoms.
If you're bleeding heavily, ask your doctor to check:
Serum ferritin (most sensitive marker of iron stores — should ideally be >50 ng/mL)
Complete blood count (hemoglobin and hematocrit — to check for anemia)
Serum iron, transferrin saturation, TIBC (for a complete iron picture)
If you're deficient:
Iron bisglycinate is the gentlest, best-absorbed supplement form
Take with vitamin C to enhance absorption
Avoid taking with calcium, coffee, or tea (they inhibit absorption)
Recheck ferritin after 3 months of supplementation
Severe deficiency may require IV iron infusion for faster repletion
Nutritional support for blood production:
Iron-rich foods: red meat, organ meats, lentils, spinach, pumpkin seeds, dark chocolate
Vitamin B12 and folate: essential for red blood cell production
Vitamin C: enhances non-heme iron absorption — pair with iron-rich meals
When to Consider Further Investigation
Your doctor may recommend further investigation if:
Heavy bleeding doesn't respond to first-line treatment
Ultrasound shows endometrial thickening (>12–16mm in perimenopause, though thresholds vary)
Structural abnormalities are suspected (fibroids, polyps)
You have risk factors for endometrial hyperplasia or cancer
Bleeding patterns are atypical for your clinical picture
Investigations may include:
Transvaginal ultrasound — to assess endometrial thickness and uterine structure
Saline infusion sonohysterography (SIS) — ultrasound with saline injected into the uterus for clearer visualization
Endometrial biopsy — sampling of the uterine lining, done in the office
Hysteroscopy — a camera inserted into the uterus for direct visualization and potential treatment
These procedures sound intimidating but are generally well-tolerated, quick, and highly informative. They provide the information needed to either reassure you or catch and treat conditions early.
Contraception During Perimenopause — The Conversation Most Women Forget
Yes, You Can Still Get Pregnant
This is the statement that surprises many women:
You can conceive during perimenopause.
As long as you are still ovulating — even sporadically — pregnancy is possible. And because ovulation is unpredictable during perimenopause, you may ovulate in a month when you "didn't expect it."
Statistics:
Fertility declines significantly after 40 — but it doesn't reach zero until menopause
Unintended pregnancies in women over 40, while less common, do occur — and carry higher medical risks than pregnancies at younger ages
You cannot confirm that you've stopped ovulating based on irregular periods alone
The rule: Contraception should be used until:
Age 55 (regardless of bleeding pattern) — per FSRH guidelines
OR 2 years after your last period if you're under 50
OR 1 year after your last period if you're over 50
Contraception Options That Also Help Symptoms
Several contraceptive methods offer dual benefits during perimenopause — preventing pregnancy while also managing symptoms:
When You Can Safely Stop Contraception
If under 50: Continue contraception until 2 years after your last natural period
If over 50: Continue contraception until 1 year after your last natural period
If over 55: Contraception can generally be stopped, as natural conception at this age is extremely rare
Important: If you're using a hormonal IUD or hormonal contraception that suppresses periods, you may not know when your natural periods have stopped. In this case, discuss with your provider — FSH testing (done twice, 6 weeks apart, while temporarily off hormonal contraception) can sometimes help determine menopausal status, though it's not perfectly reliable.
Your Period Is Telling You a Story — Here's How to Listen
Your menstrual cycle during perimenopause isn't just a symptom to manage. It's information.
Every change — every shortened cycle, every flood, every skipped month — is your body communicating its hormonal state. When you track these changes, you're not just gathering data for your doctor. You're reading your own biology in real time.
Here's what your period might be telling you:
Shorter cycles: "I'm working harder. Ovulation is accelerating. The early transition has begun."
Heavier periods: "I'm not ovulating consistently. Estrogen is building the lining without progesterone's reset. The transition is active."
Skipped months: "I'm ovulating less and less. The late transition is underway."
Spotting between periods: "My hormones are fluctuating. The lining is unstable. I'm in flux."
Longer gaps: "I'm approaching the end. But I'm not there yet."
Nothing for months, then surprise: "Don't count me out. This transition has its own timeline."
Your period has been your companion for decades. During perimenopause, it's not abandoning you — it's winding down. And if you listen to what it's telling you, you'll navigate the transition with more clarity, less anxiety, and better care.
You know your body. Trust that knowledge. Track the changes. Seek help when the red flags appear. And for everything else — breathe. This is normal. This is temporary. And you are not alone.
FAQ — Irregular Periods in Perimenopause
Q: Are irregular periods normal during perimenopause?
A: Yes. Irregular periods are the hallmark of perimenopause — including shorter or longer cycles, heavier or lighter bleeding, skipped months, and unpredictable timing. These changes are driven by fluctuating hormones and inconsistent ovulation, and are expected during the transition.
Q: When should I worry about irregular periods in perimenopause?
A: See your doctor if you're soaking through protection every hour, bleeding lasts more than 10 days, you have bleeding after sex, or bleeding returns after 12+ months without a period. Also seek evaluation if you have symptoms of anemia — fatigue, dizziness, breathlessness.
Q: Can perimenopause cause very heavy periods?
A: Yes. Heavy periods are common in perimenopause, caused by anovulatory cycles where the uterine lining builds without progesterone's regulating effect. Up to 25–30% of women experience prolonged or very heavy bleeding during the transition.
Q: Can you still get pregnant during perimenopause?
A: Yes. As long as you're still ovulating — even sporadically — pregnancy is possible. Contraception should be used until age 55, or until 1–2 years after your last natural period (depending on age). Consult your provider for guidance.
Q: How do I know when my periods are ending for good?
A: Menopause is confirmed after 12 consecutive months without a menstrual period. Before that, periods may stop for weeks or months and then return — this is normal. Lengthening gaps between periods (60–90+ days) suggest you're approaching the end.
Q: Should I take iron if my periods are heavy during perimenopause?
A: Only after testing confirms deficiency. Ask your doctor to check serum ferritin, which should ideally be above 50 ng/mL. Iron bisglycinate is the gentlest supplement form. Never supplement iron without testing first — excess iron can be harmful.
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References
Perimenopause Compass
Contact
hello@perimenopausecompass.com
© 2026 All rights reserved.