Why Perimenopause Feels So Overwhelming (And What's Actually Happening)
Perimenopause doesn't just bring symptoms — it brings a storm. Learn why perimenopause feels so overwhelming, what's really happening in your brain and body, and how to find your footing again.
EDUCATIONAL
3/17/202623 min read
You're standing in your kitchen. The dishes are piled up. Your teenager needs something. Your work email is pinging. Your hip aches. You slept four hours. Your heart is doing that thing again. You're hot — then cold. You forgot what you came into the room for. You're not sure whether you're about to cry, scream, or sit on the floor and do absolutely nothing.
And underneath all of it, one thought keeps circling:
What is happening to me?
Not "what are my symptoms" — you can list those. Not "what stage am I in" — you've read the articles. But the bigger question. The one that rises at 3 a.m. and presses against your chest at 2 p.m.:
Why does this feel like so much? Why can't I cope? What is wrong with me?
Nothing is wrong with you.
What's happening is that you're experiencing the most significant hormonal, neurological, and physiological recalibration of your adult life — while simultaneously navigating one of the most demanding decades of most women's lives — with almost no cultural preparation, medical support, or social permission to struggle.
That's not weakness. That's an impossible equation.
This article explains why perimenopause feels so overwhelming — not just emotionally, but biologically, neurologically, and systemically. Because once you understand what's actually happening inside you, something shifts. Not the symptoms themselves — but your relationship to them. And that changes everything.
You're Not Weak. You're Not Failing. Here's What's Really Going On.
The Question Nobody Answers
If you've been reading about perimenopause, you've probably learned about individual symptoms. Hot flashes. Insomnia. Brain fog. Anxiety. Irregular periods. Joint pain.
But here's what no article, no doctor, and no menopause checklist addresses:
Why does the whole thing feel like it's too much?
It's not one symptom. It's twenty symptoms happening simultaneously in a body that also has to parent, work, partner, caretake, perform, show up, smile, and hold it all together.
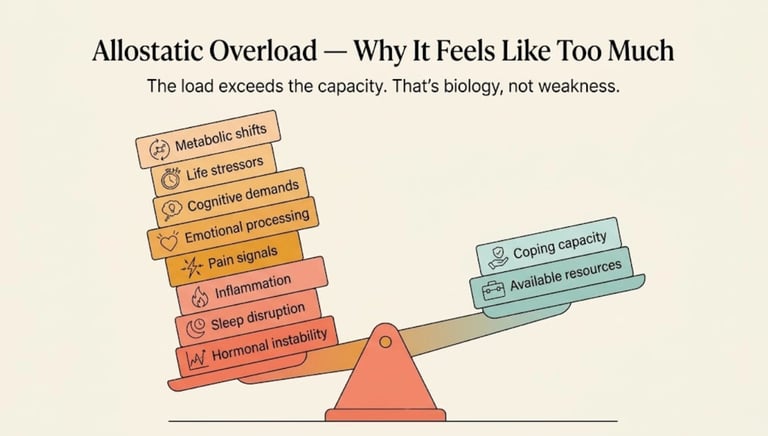
It's the cumulative weight — the pile-on — that creates the feeling of overwhelm. And it has a name, a biology, and an explanation.
Why "Just Manage Your Symptoms" Misses the Point
Most medical advice for perimenopause takes a symptom-by-symptom approach:
Hot flashes? Try HRT.
Can't sleep? Sleep hygiene.
Anxious? Consider an SSRI.
Joint pain? Anti-inflammatories.
Brain fog? More exercise.
Each piece of advice is individually reasonable. But collectively, it misses something crucial:
You're not dealing with a list of problems. You're dealing with a system under siege.
Managing individual symptoms without addressing the underlying overwhelm is like putting out small fires while the building's electrical system is short-circuiting. You need to fix the wiring — not just chase the flames.
That "wiring" is your nervous system, your brain chemistry, your stress response, your energy budget, and your capacity to cope — all of which are profoundly altered during perimenopause. And all of which are under additional strain from the life circumstances that typically surround this transition.
The Seven Reasons Perimenopause Feels Like Too Much
Reason 1 — Your Brain's Chemistry Has Changed
This is the most important thing to understand, and the thing most doctors don't explain:
Perimenopause is not just a reproductive event. It is a neurological event.
Estrogen is one of the most powerful modulators of brain chemistry. It directly influences:
Serotonin — your emotional stability and wellbeing neurotransmitter
GABA — your brain's primary calming system
Dopamine — your motivation, reward, and pleasure circuits
Norepinephrine — your alertness and stress response
Acetylcholine — your memory and learning systems
Endorphins — your natural pain-relief and mood-boosting system
When estrogen fluctuates wildly during perimenopause — spiking one day, crashing the next — all of these systems become unstable simultaneously.
This is not metaphorical. It is not psychological. It is neurochemistry — the same class of brain changes that occur in clinical depression, anxiety disorders, and neurological conditions. The difference is that in perimenopause, the changes are hormonally driven and often temporary — but while they're happening, they are profoundly real.
The result: you feel less emotionally stable, less resilient, less motivated, more anxious, more reactive, less sharp, and less like yourself. Not because you're weaker. Because your brain's operating chemicals have become unreliable.
Reason 2 — Your Nervous System Is in Overdrive
Your autonomic nervous system (ANS) — the system that runs your fight-or-flight response, heart rate, temperature, digestion, and arousal — is estrogen-sensitive and becomes dysregulated during perimenopause.
What this looks like from the inside:
Your fight-or-flight system (sympathetic nervous system) activates more easily and more often — creating a background state of hypervigilance
Your rest-and-digest system (parasympathetic nervous system) has trouble engaging — making it harder to calm down, sleep deeply, or feel safe
Small stressors that you used to absorb without noticing now feel like major threats
Your body exists in a state of chronic low-level alarm — not because anything terrible is happening, but because the nervous system's calibration has shifted
This is why:
A work email that would have been mildly annoying now triggers a cascade of anxiety
A disagreement with your partner feels catastrophic instead of normal
A busy day that you would have powered through now leaves you completely depleted
You can't "just relax" even when you try — because your nervous system isn't cooperating
You don't have a coping problem. You have a nervous system that has lost its brakes.
Reason 3 — Your Body Is Sending Alarms from Every System
As we've detailed in our body systems article, estrogen receptors exist in nearly every tissue. During perimenopause, every system can send distress signals:
Your joints ache
Your gut is unpredictable
Your skin burns or itches
Your heart races
Your brain fogs
Your muscles twitch
Your temperature swings
Each signal, individually, would be manageable. But your brain isn't receiving one alarm — it's receiving signals from every direction, simultaneously, all day, every day.
This is like trying to work while every fire alarm in the building is going off, in different rooms, at unpredictable intervals. Your brain is spending so much energy processing internal signals that it has almost nothing left for the external demands of your life.
This is interoceptive overload — and it is a real, documented neurological state. It explains why even simple decisions feel exhausting, why your tolerance for stimulation has plummeted, and why you feel "full" even when you haven't done much.
Reason 4 — Your Sleep Has Been Stolen
Sleep deprivation alone — even without hormonal changes — causes:
Impaired emotional regulation
Reduced cognitive function
Increased pain sensitivity
Elevated stress hormones (cortisol)
Weakened immune function
Reduced ability to cope with adversity
Now layer perimenopausal sleep disruption onto this:
Night sweats waking you multiple times
3 a.m. awakenings with racing thoughts (cortisol surges)
Lighter, less restorative sleep architecture (less deep and REM sleep)
Difficulty falling back asleep once woken
Feeling unrested regardless of hours in bed
The result: you're navigating the most complex hormonal transition of your adult life on a fraction of the sleep your brain and body need to function.
Sleep deprivation is an amplifier. It takes every symptom — physical, emotional, cognitive — and turns up the intensity. It is often the single most impactful factor in the "overwhelm equation," and addressing it should be the first priority in any management strategy.
Reason 5 — You're Carrying an Invisible Load
Perimenopause doesn't happen in a vacuum. It happens during one of the most demanding decades of most women's lives:
The professional load:
Career demands that are often at their peak
The pressure to perform, lead, and deliver — while your brain fog makes you forget the word you need mid-presentation
The caregiving load:
Aging parents who need increasing support
Teenagers or young adults who need emotional and practical guidance
Sometimes both — the "sandwich generation" reality
The domestic load:
The mental load of running a household — planning, organizing, remembering, anticipating
Emotional labor — managing the emotional needs of partners, children, parents, friends
The invisible work that keeps everything functioning — and that nobody sees or credits
The health load:
Managing your own perimenopause (appointments, research, tracking, advocating)
Possibly managing a partner's or parent's health issues
Navigating a healthcare system that may dismiss or minimize your experience
The identity load:
Processing changes in your body, appearance, energy, and capacity
Confronting cultural messages about aging, desirability, and value
Grieving the version of yourself that seemed to handle everything effortlessly
Each of these loads, individually, would be manageable with a fully resourced brain and body. Combined — and layered onto hormonal, neurological, and sleep disruptions — they create a weight that exceeds your current capacity. Not because your capacity is small, but because the load is enormous and your resources are temporarily depleted.
Reason 6 — Your Identity Is Shifting
This one is rarely discussed in medical contexts, but it's one of the most significant contributors to overwhelm:
Perimenopause isn't just a physical transition. It's an identity transition.
You are moving from one phase of life to another — and that movement involves loss, uncertainty, and reinvention:
Loss of the body that used to be reliable
Loss of the cognitive sharpness you took for granted
Loss of the reproductive capacity that, whether or not you wanted more children, was part of your identity as a biological woman
Loss of the version of yourself that could do it all, handle it all, be everything to everyone
Uncertainty about who you're becoming — what this next phase holds, what you'll look like, feel like, be like
Reinvention — the invitation (or forced requirement) to reassess your priorities, boundaries, relationships, and definition of self
Identity transitions are inherently disorienting. They consume psychological energy. They create a sense of groundlessness — the feeling that you don't quite know who you are right now, even though you've known yourself for decades.
This isn't self-indulgent navel-gazing. It's a developmental passage — as significant as adolescence, though far less acknowledged.
Reason 7 — Nobody Prepared You for This
Perhaps the most enraging contributor to overwhelm:
You were given almost no preparation for this experience.
Your mother likely didn't talk about it
Your doctor probably didn't mention it until you asked
Your school education covered puberty, periods, and pregnancy — but not what happens when all of that ends
Cultural narratives about menopause are dominated by jokes, silence, or dread
Medical training devotes a few hours to menopause across the entire curriculum
The result: when perimenopause hits, you have no framework. No map. No cultural wisdom. No normalizing stories. Just symptoms and silence.
This means every symptom triggers additional anxiety — "Is this normal? Is something wrong? Am I the only one? Should I be worried?" — that wouldn't exist if you'd been educated and prepared.
The overwhelm of perimenopause is not just physiological. It's compounded by an information vacuum that turns a manageable transition into a bewildering crisis.


What Women Actually Experience — The Overwhelm Nobody Warns You About
"I Used to Handle Everything. Now I Can Barely Handle Tuesday."
"I was the woman who ran the department, coached the kids' soccer team, hosted dinner parties, and still had energy for the gym. Now I spend Sunday nights in dread of Monday morning. I've started canceling plans because the thought of being 'on' for two hours is more than I can face. My capacity has shrunk — dramatically, visibly, embarrassingly. And the worst part is that nobody understands. They see me and think I'm fine. I look fine. I'm NOT fine. I'm running on empty in a life that was designed for a full tank."
"I Feel Like I'm Drowning in Shallow Water"
"That's the most accurate description I've found. The water isn't deep. The individual demands of my life aren't extraordinary. Nothing objectively terrible is happening. But I'm drowning anyway — because my ability to keep my head above water has been halved. Every breath takes more effort. Every stroke forward is harder. And from the outside, people just see someone standing in water that barely reaches their waist. 'Why can't you just stand up?' Because my legs don't work the way they used to."
"The Worst Part Isn't Any Single Symptom — It's ALL of Them at Once"
"I could handle the hot flashes. I could handle the insomnia. I could handle the brain fog. I could handle the anxiety. I could handle the joint pain. I could EVEN handle the weird skin crawling thing. But I can't handle ALL OF THEM AT ONCE. It's the accumulation. The stacking. The fact that there is no system in my body that is working normally right now. I am fighting fires on every front — with no backup, no sleep, and a brain that won't cooperate."
"I Don't Recognize Myself Anymore"
"I used to be patient. I used to be calm. I used to be sharp. I used to be funny. I used to be energetic. I used to be confident. I used to be curious. I look in the mirror and see someone familiar but altered — like a photo of myself with the contrast changed. Same person, different quality. And I grieve for who I was — even though I know she's still in there somewhere. She's just buried under hormonal rubble. And some days, I can't find her at all."
What Science Says — The Biology of Overwhelm
Allostatic Load — When Your System Can't Keep Up
The concept of allostatic load — developed by neuroscientist Bruce McEwen — provides the most accurate scientific framework for understanding perimenopausal overwhelm.
Allostasis is your body's ability to maintain stability through change — to adapt to stressors by adjusting internal systems (cortisol, blood pressure, heart rate, immune function, etc.).
Allostatic load is what happens when the demands on these systems exceed their capacity to adapt — when the stressors pile up faster than your body can recalibrate.
During perimenopause, your allostatic load increases from multiple directions simultaneously:
When allostatic load exceeds capacity, the system doesn't just struggle — it changes how it operates:
Stress hormones stay elevated chronically (instead of spiking and recovering)
Sleep architecture degrades further (less deep sleep, more fragmented)
Pain sensitivity increases (central sensitization)
Emotional reactivity increases (the amygdala becomes hyperactive)
Cognitive function declines (the prefrontal cortex has less energy available)
Immune function becomes dysregulated (more inflammation, more susceptibility)
This is why you feel like you're drowning in shallow water. The water isn't deep. But your capacity to swim has been reduced by a system under more strain than it was designed to handle simultaneously.
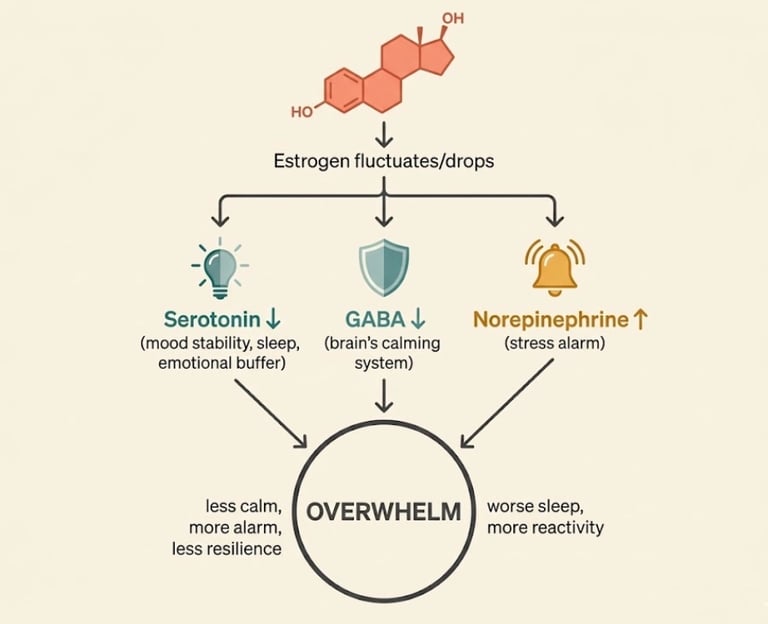
The Estrogen-Serotonin-GABA Cascade
This is the neurochemical cascade at the heart of perimenopausal overwhelm:
Estrogen drops → serotonin production decreases
Less emotional stability
More anxiety and depression vulnerability
Reduced ability to modulate stress responses
Poorer sleep (serotonin is a precursor to melatonin)
Estrogen drops → GABA activity decreases
GABA is your brain's primary "calming" neurotransmitter
Less GABA = reduced ability to stop anxiety, quiet racing thoughts, relax muscles, and transition into deep sleep
Your brain's natural "off switch" becomes unreliable
Estrogen drops → norepinephrine becomes more reactive
Norepinephrine is your alertness/alarm neurotransmitter
More norepinephrine reactivity = more hypervigilance, more startle response, more physical anxiety symptoms (racing heart, tight chest, shallow breathing)
Combined effect:
Less calming (serotonin ↓, GABA ↓)
More alarming (norepinephrine ↑)
Less emotional resilience
More physical anxiety sensations
Poorer sleep
Greater vulnerability to overwhelm
This is not a metaphor. This is documented receptor biology and neuropharmacology. The same cascade explains why SSRIs (which increase serotonin) and benzodiazepines (which enhance GABA) are sometimes prescribed in perimenopause — and why HRT, which stabilizes the upstream cause (estrogen), often resolves the downstream effects more comprehensively.
The HPA Axis — Your Stress System Has Lost Its Brakes
Your HPA axis (Hypothalamic-Pituitary-Adrenal axis) is your body's central stress response system. It controls cortisol — your primary stress hormone.
In a well-functioning system:
Stress occurs → cortisol rises → you respond → cortisol comes back down
The system has negative feedback — like a thermostat that turns off when the room is warm enough
During perimenopause:
Estrogen normally helps regulate HPA axis sensitivity — keeping the thermostat calibrated
As estrogen fluctuates, the HPA axis becomes more reactive and less self-regulating
Cortisol spikes more easily, rises higher, and stays elevated longer
The "thermostat" doesn't turn off properly
Over time, the system can become tonically activated — you're running on stress hormones even when nothing stressful is happening
This is why you feel wired but tired, why you can't relax even when you try, and why your body feels like it's operating in permanent emergency mode.
The cortisol dysregulation also feeds back into the overwhelm cycle:
Elevated cortisol → worse sleep → more fatigue → less coping capacity → more overwhelm → more cortisol
Elevated cortisol → increased inflammation → more joint pain, more brain fog → more overwhelm → more cortisol
Elevated cortisol → impaired prefrontal cortex function → worse decision-making, more emotional reactivity → more overwhelm → more cortisol
It's a loop. And breaking the loop requires addressing the system — not just individual symptoms.
Central Sensitization — When the Volume Won't Turn Down
As discussed in our weird symptoms article, central sensitization is a neurological state where your brain amplifies sensory signals — making normal inputs feel abnormal, uncomfortable, or overwhelming.
During perimenopause, central sensitization contributes to overwhelm by:
Making sounds, lights, and touch feel more intense than they should
Making pain signals from joints, muscles, and viscera feel more severe
Making internal body sensations (heartbeat, digestion, breathing) more consciously prominent
Reducing your tolerance for stimulation — crowded spaces, busy environments, multi-tasking
The result: your subjective experience of the world is louder, harsher, and more demanding than it objectively is. You're not being dramatic. Your nervous system has literally turned up the volume — and you can't turn it back down with willpower alone.
The Prefrontal Cortex Under Siege
Your prefrontal cortex (PFC) is the brain region responsible for:
Executive function — planning, organizing, prioritizing, decision-making
Emotional regulation — managing reactions, maintaining perspective, impulse control
Working memory — holding information in mind while using it
Cognitive flexibility — shifting between tasks, adapting to change
The PFC is highly energy-dependent — it requires stable glucose, adequate sleep, and neurochemical support (serotonin, dopamine, GABA) to function optimally.
During perimenopause, every one of these supports is compromised:
Sleep deprivation → PFC energy depletion
Blood sugar instability → unreliable glucose supply
Serotonin/GABA fluctuations → neurochemical instability
Chronic cortisol → PFC structural and functional changes (cortisol is neurotoxic to the PFC at chronically elevated levels)
Inflammation → reduces PFC efficiency
This is why:
Decisions that used to be automatic now feel paralyzing
You can't prioritize — everything feels equally urgent
You react emotionally before your rational mind catches up
You forget things that are right in front of you
Multi-tasking — which you used to do effortlessly — is now nearly impossible
You feel "stupid" — when you're actually experiencing PFC depletion, not cognitive decline
The irony: perimenopause demands MORE executive function (managing symptoms, navigating medical appointments, tracking cycles, adjusting routines, processing emotional change) at precisely the moment you have LESS of it available. This mismatch is one of the deepest sources of overwhelm.
What's Established vs. What We're Still Learning
Scientifically established:
Estrogen directly modulates serotonin, GABA, dopamine, and norepinephrine
The HPA axis becomes more reactive during the menopausal transition
Sleep disruption amplifies every symptom domain
Cognitive function (especially executive function and verbal memory) is affected during the transition
Allostatic load increases during perimenopause from multiple converging sources
Central sensitization can be hormonally modulated
Probable (growing evidence):
The degree of hormonal fluctuation (not just decline) may predict overwhelm severity
Gut microbiome changes during perimenopause contribute to systemic inflammation and mood
Prior adverse childhood experiences or trauma may increase vulnerability to perimenopausal overwhelm through HPA axis sensitization
The timing and type of intervention (HRT, CBT, nervous system work) may matter more than previously recognized
Still debated or under-researched:
Whether specific personality traits or neurobiological profiles predict perimenopausal overwhelm
The optimal combination of interventions for global overwhelm (vs. individual symptom management)
The long-term cognitive implications of chronic perimenopausal stress
How cultural and socioeconomic context modifies the overwhelm experience
This article is for educational purposes and does not replace medical advice. If you're experiencing overwhelming symptoms, consult a healthcare provider — ideally one with expertise in menopause medicine.
The Perfect Storm — Why Everything Converges at Once
Perimenopause doesn't just feel like a lot because of what's happening inside your body. It feels like a lot because everything converges at the same time.
The Hormonal Storm
Your hormones are in flux — estrogen spiking and crashing, progesterone declining, testosterone gradually dropping. This creates neurochemical instability, thermoregulatory chaos, inflammatory shifts, and metabolic changes. Every body system is affected. Every day is different. There's no stable ground to stand on.
The Life-Stage Storm
Perimenopause typically hits during the peak complexity decade of most women's lives:
Children who need you most (teenagers or young adults in critical phases)
Parents who are aging and increasingly dependent
Career demands at their highest (leadership, institutional knowledge, performance pressure)
Financial pressures (education costs, mortgage, retirement planning)
Relationship dynamics that may have calcified or need renegotiation
You don't get to step out of your life while your body recalibrates. You have to keep functioning — at the same level as before — with significantly fewer internal resources.
The Relationship Storm
Perimenopause can stress even the strongest relationships:
Libido changes create distance and guilt
Mood volatility creates conflict and walking-on-eggshells dynamics
Your partner's confusion (not understanding what's happening) can feel like abandonment
Communication gaps widen when you can't articulate what you're feeling (because you don't fully understand it yourself)
Partners may be experiencing their own midlife changes simultaneously
The Identity Storm
As described above — the loss, the uncertainty, the reinvention. You're not just managing symptoms. You're processing the existential question of who you are becoming — and whether you can grieve who you were.
The Cultural Storm
A culture that equates women's value with youth, beauty, and productivity
A medical system that minimizes or dismisses women's symptoms
A workplace that has no framework for supporting hormonal transitions
Social media that presents midlife women as either "thriving" or invisible
The persistent message: keep going, keep smiling, keep performing
Why the Convergence Makes Each Part Feel Worse
This is the crucial insight: these storms don't just add up — they multiply.
Sleep deprivation makes hormonal symptoms more severe. Hormonal symptoms worsen cognitive function. Reduced cognitive function impairs your ability to manage your workload. Work stress elevates cortisol. Cortisol worsens sleep. And around you go.
Each storm intensifies every other storm. The convergence creates a compound effect that is greater than the sum of its parts.
This is why perimenopause feels like "too much" — because it IS too much, for a system operating under these combined conditions. The overwhelm is not a failure of character. It's an accurate reflection of compound load on a depleted system.
Why It Feels Like You're Falling Apart (But You're Not)
The Difference Between Breaking Down and Breaking Through
Here's a reframe that many women in perimenopause eventually discover:
What feels like breaking down is often the beginning of breaking through.
Perimenopause strips away the margins. The buffer zone you used to have — the extra energy, the extra patience, the extra capacity to absorb stress without showing it — disappears.
And what's revealed when the margins are gone? The unsustainable patterns that were hiding underneath:
The over-functioning you've been doing for decades
The boundaries you never set because you had the energy to work around them
The relationships that were consuming more than they were giving
The standards of performance you held yourself to that were never realistic
The "I'm fine" autopilot that was keeping everything running at the cost of your wellbeing
Perimenopause doesn't create these patterns. It exposes them — by removing the hormonal buffer that allowed you to sustain them.
This exposure is painful. It feels like collapse. But it's also an invitation — sometimes the only invitation your body knows how to send — to rebuild on more sustainable foundations.
What Perimenopause Actually Reveals
Many women, looking back from the other side, describe perimenopause as the time when they were forced to:
Learn to say no
Let go of perfectionism
Ask for help (genuinely, not performatively)
Prioritize themselves — not as a luxury but as a necessity
Renegotiate relationships that weren't serving them
Confront the question: "What do I actually want from my next chapter?"
This isn't "silver lining" toxic positivity. You shouldn't have to go through hormonal chaos to learn these lessons. But the reality is: many women do. And the lessons, once learned, often become the foundation for a more authentic, more boundaried, and ultimately more satisfying second half of life.
The Recalibration Metaphor — Your Operating System Is Updating
Think of perimenopause as your body's operating system update.
Your previous OS (estrogen-dominant, premenopausal) ran smoothly for decades. It supported everything — your energy, your mood, your cognition, your temperature, your joints, your sleep, your reproductive function.
Now, your body is migrating to a new OS (postmenopausal). The new system will be stable — but the migration process is messy. During the update:
Apps crash (symptoms)
Processing slows (brain fog)
The system overheats (hot flashes)
Battery drains faster (fatigue)
Some features temporarily stop working (sleep, mood regulation)
Error messages appear constantly (somatic symptoms)
The update cannot be rushed. But it can be supported — with the right tools, the right environment, and the right understanding.
And when it's complete? The new OS is different — but it works. Many women describe postmenopause as a time of stability, clarity, and renewed energy that they couldn't have imagined during the chaos of the transition.
What Actually Helps — Not Just Symptom Management, But System Support
The interventions below are designed to address the whole system — not just individual symptoms. They work on the nervous system, the stress response, the inflammation cascade, the sleep architecture, and the cognitive and emotional infrastructure that perimenopause has disrupted.
Step 1 — Name It (And Stop Blaming Yourself)
The most immediately powerful intervention is cognitive:
Stop telling yourself something is wrong with you. Start telling yourself: "My system is under unprecedented load, and the overwhelm I feel is a biologically appropriate response."
This reframe doesn't eliminate symptoms. But it does two things:
It stops the shame spiral — guilt and self-blame consume enormous psychological energy. Releasing them frees resources for actual coping.
It changes your relationship to the experience — you move from "I'm broken" to "I'm navigating something real" — which is fundamentally more empowering and less overwhelming.
Step 2 — Protect Your Sleep Like Your Life Depends on It
Sleep is the single most impactful variable in the overwhelm equation. Improving sleep improves everything else — mood, cognition, pain tolerance, emotional regulation, hormone balance, immune function.
What to prioritize:
CBT-I (Cognitive Behavioral Therapy for Insomnia) — the gold standard non-drug treatment for insomnia. Specifically effective for perimenopausal insomnia. Available as programs, apps (Sleepio), or with a trained therapist.
Sleep environment optimization — cool room (60–67°F / 15–19°C), moisture-wicking bedding, blackout conditions, consistent schedule
HRT — if vasomotor symptoms (night sweats, hot flashes) are disrupting sleep, HRT can be transformative. Progesterone in particular has sedative properties and can significantly improve sleep quality
Magnesium glycinate (200–400 mg before bed) — modest but positive evidence for sleep support
Limiting alcohol — even one drink can fragment sleep architecture, worsen night sweats, and increase 3 a.m. awakenings
Caffeine cutoff — no caffeine after noon. Sensitivity increases during perimenopause.
Step 3 — Regulate Your Nervous System Daily
Your ANS needs daily intentional downregulation — you cannot willpower your way out of a nervous system stuck in overdrive. But you can give it physiological signals that activate the calming (parasympathetic) branch:
Daily practices (10–20 minutes total):
Extended exhale breathing — inhale for 4 counts, exhale for 7–8 counts. This directly activates the vagus nerve and parasympathetic system. The single most accessible nervous system intervention.
Cold water on the face or wrists — triggers the mammalian dive reflex, immediately lowering heart rate and activating the vagal brake.
Gentle movement — walking (especially in nature), yoga, tai chi, stretching. NOT high-intensity (which can further stress an already-activated system).
Humming or singing — vibrates the vagus nerve in the throat, signaling safety to the brainstem.
Progressive muscle relaxation — systematic tension/release of muscle groups, reducing the background muscular tension that keeps your nervous system on alert.
The key: Consistency beats intensity. Five minutes of breathing twice a day is more effective than one 30-minute meditation once a week. Your nervous system needs regular, repeated signals that it's safe to stand down.
Step 4 — Reduce the Load (Ruthlessly)
If your allostatic load exceeds your capacity, the most logical intervention is to reduce the load.
This is the step most women resist — because the load feels non-negotiable. But some of it IS negotiable if you give yourself permission:
Ask yourself:
What can I delegate? (To a partner, a child, a colleague, a service)
What can I defer? (Projects, commitments, obligations that don't have a true deadline)
What can I decline? (Invitations, requests, volunteer commitments, optional meetings)
What can I drop entirely? (Standards of perfection, tasks that don't actually matter, activities that drain more than they give)
The perimenopause triage question:
For every commitment, ask: "Given my current capacity, is this essential, important, or optional?"
Essential: do it.
Important: do it if you can — delegate if you can't.
Optional: let it go.
This is not laziness. This is strategic resource management during a period of reduced capacity. CEOs do it when their companies are under stress. Athletes do it when their bodies are recovering. You are allowed to do it when your entire biological system is in transition.
Step 5 — Nourish the Infrastructure
Your brain and nervous system need specific nutritional support during perimenopause — the same way a building under renovation needs scaffolding:
Protein at every meal (25–35g) — provides the amino acids that are precursors to serotonin, dopamine, and GABA
Omega-3 fatty acids — anti-inflammatory, neuroprotective, mood-supporting. From fatty fish or supplementation (1,000–2,000 mg EPA/DHA)
Complex carbohydrates — needed for serotonin production (don't cut carbs too low — it can worsen mood and sleep)
Magnesium — supports GABA, muscle relaxation, sleep, and nervous system calm. Most women are deficient
B vitamins — support energy metabolism and neurotransmitter production. Methylated forms preferred
Stable blood sugar — eat regular meals. Pair carbs with protein and fat. Avoid prolonged fasting if you're prone to crashes
Reduced alcohol — alcohol worsen sleep, inflammation, anxiety, and hormonal instability. Reducing or eliminating it is often the single most impactful dietary change
Step 6 — Get Medical Support (You've Earned It)
Medical intervention is not a last resort. It's a legitimate, evidence-based tool that can dramatically reduce overwhelm:
HRT — stabilizes the upstream cause (estrogen fluctuations) that drives the downstream cascade (neurochemistry, sleep, inflammation, cognition, mood). Many women describe starting HRT as "getting myself back." It's not a magic pill — but for many, it's the closest thing to one.
CBT or therapy — cognitive behavioral therapy for insomnia, anxiety, or general psychological support. Particularly valuable for the identity and existential dimensions of overwhelm.
Antidepressants — if mood symptoms are severe, an SSRI or SNRI can help. Bupropion (Wellbutrin) is an option that doesn't suppress libido and may help energy.
Progesterone — micronized progesterone can specifically improve sleep and anxiety (enhances GABA).
What to tell your doctor:
"I'm experiencing perimenopausal overwhelm — not just individual symptoms, but a cumulative burden that's exceeding my ability to cope. I'd like to discuss comprehensive support, including HRT if appropriate, and I'd like a referral to a menopause specialist if needed."
Step 7 — Build Your Circle
Isolation amplifies overwhelm. Connection reduces it.
Find your people — other women in perimenopause who understand. Online communities, support groups, friends going through the same transition.
Educate your inner circle — share articles (like this one) with your partner, close friends, or family. Let them see what you're navigating.
Professional support — a therapist, a coach, a menopause-informed practitioner. Someone in your corner who understands.
Reduce exposure to people who drain you — perimenopause is a clarifying fire. It shows you who fills your cup and who empties it. Act accordingly.
What to Say to the People Who Don't Understand
To Your Partner
"I need you to understand that what I'm going through isn't mood swings or bad days. My brain chemistry has changed. My nervous system is in overdrive. My body is sending alarm signals from every system. I'm not choosing to be overwhelmed — I'm experiencing a biological storm, and I need your patience, your belief, and your help. Not because I'm weak — because this is genuinely hard, and I can't do it alone."
You might also share: "Please read [this article] — it explains what's happening in my brain and body better than I can right now. I need you to understand this the way you'd understand if I was recovering from a surgery or managing a chronic condition. Because that's closer to the reality than 'she's just stressed.'"
To Your Employer or Colleagues
"I'm navigating a health transition that's temporarily affecting my energy, concentration, and capacity. I'm managing it proactively, and I may need some flexibility around [specific requests — adjusted meeting times, quiet workspace, flexible deadlines for non-critical work]. This is a temporary phase, not a permanent change in my capability."
Note: You are not obligated to disclose that it's perimenopause. In the UK, menopause is increasingly recognized under workplace health policies; in the US, the framework is less established. Disclose only what you're comfortable with and only if it serves you.
To Yourself
"I am not broken. I am not failing. I am navigating a biological transition of enormous complexity — with less sleep, less neurochemical stability, and more demands than my system was designed to handle simultaneously. The overwhelm I feel is not a character flaw. It is an accurate signal that my load exceeds my current capacity. And that's not a permanent state — it's a temporary imbalance that can be addressed, managed, and eventually resolved."
"I deserve support. I deserve understanding. I deserve to lower the bar while my system recalibrates. And I deserve to come through this knowing that I didn't just survive — I adapted."
The Truth About the Other Side
We can't promise that perimenopause will be easy. It's not. It's one of the hardest things many women experience — precisely because it's compound, invisible, under-recognized, and relentless.
But we can tell you what the research shows, and what millions of women who've crossed to the other side report:
The storm calms.
Hormones stabilize. The nervous system recalibrates. Sleep returns. Cognition clears. The emotional ground becomes firm again.
And many women — not all, but many — describe postmenopause as a time of:
Greater clarity — about what matters and what doesn't
Stronger boundaries — learned through necessity during the transition
Deeper self-knowledge — forged in the fire of identity disruption
Less tolerance for what doesn't serve them — a gift disguised as a symptom
Renewed energy — different from the energy of their 30s, but real and sustained
A sense of having survived something — and being fundamentally strengthened by it
This isn't guaranteed. And it's not helpful to hear when you're in the worst of it. But it's true. And sometimes, on the hardest days, knowing that there IS another side — even if you can't see it yet — is enough to keep going.
You will come through this. Not the same person you were before. But whole. Recalibrated. And, in many ways, more yourself than you've ever been.
FAQ — Why Perimenopause Feels So Overwhelming
Q: Why does perimenopause feel so overwhelming?
A: Perimenopause creates simultaneous disruption across multiple body systems — brain chemistry (serotonin, GABA), nervous system regulation, sleep architecture, inflammation, and cognition — while typically coinciding with peak life demands. The compound effect exceeds normal coping capacity, creating biological overwhelm.
Q: Is perimenopausal overwhelm just stress?
A: No. While stress contributes, perimenopausal overwhelm has distinct biological drivers: estrogen-mediated changes in neurotransmitters, HPA axis dysregulation, central sensitization, and prefrontal cortex depletion. It's a neurobiological state, not a psychological weakness.
Q: Will the overwhelm go away?
A: For most women, yes. The overwhelm of perimenopause is driven by hormonal instability — once hormones stabilize after menopause (or with HRT), the nervous system recalibrates and capacity typically returns. The timeline varies, but the transition is temporary.
Q: Does HRT help with feeling overwhelmed?
A: Often, yes — sometimes significantly. HRT stabilizes estrogen, which directly supports serotonin, GABA, and nervous system regulation. Many women report that HRT reduced not just individual symptoms but the overall sense of overwhelm. Discuss with a menopause-informed provider.
Q: How can I explain perimenopause overwhelm to my partner?
A: Frame it as a biological event, not a mood issue: "My brain chemistry and nervous system have changed due to hormonal shifts. This affects my sleep, emotions, cognition, and physical comfort simultaneously. I need your understanding and support — not solutions, but partnership."
Q: When should I seek help for perimenopausal overwhelm?
A: Seek help if overwhelm is significantly affecting your ability to function at work or home, if you're experiencing persistent low mood or anxiety, if sleep disruption is chronic, or if you're having thoughts of self-harm. You don't need to reach crisis point to deserve support — early intervention is more effective.
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References
Perimenopause Compass
Contact
hello@perimenopausecompass.com
© 2026 All rights reserved.