Weird Perimenopause Symptoms Nobody Talks About
Electric shocks, burning tongue, crawling skin, tinnitus — these weird perimenopause symptoms are real and hormonal. Discover 20+ obscure symptoms nobody warns you about and why they happen.
LIFESTYLE
3/2/202631 min read
You Googled it at midnight. Maybe it was "electric shock feeling in head." Or "skin crawling sensation no rash." Or "can perimenopause cause ringing in ears." Or "why does my tongue burn for no reason."
You scrolled through medical forums. You checked WebMD and scared yourself. You asked Reddit. You wondered if you had a neurological disease, an autoimmune condition, or early-onset something terrible.
And then — maybe — buried in a comment, in a support group, in one line of one article — someone mentioned perimenopause.
And you thought: wait. Could all of this be hormonal?
Yes. Almost certainly, yes.
Welcome to the obscure symptomatology of perimenopause — the collection of strange, unsettling, bizarre, and medically under-recognized symptoms that affect millions of women during the hormonal transition and are almost never listed on the "classic symptoms" checklist.
These aren't hot flashes. They aren't missed periods. They're the symptoms that make you feel like your body has been hijacked by a stranger — the ones that send you to specialists who find nothing, the ones that wake you at 3 a.m. with a sensation you can't even name, the ones that make you wonder if you're losing your mind.
You're not losing your mind. Your nervous system is recalibrating in response to one of the most significant hormonal shifts of your life. And these symptoms — all of them — have biological explanations.
This article covers 25+ obscure perimenopause symptoms organized by body system, explains the science behind each one, tells you when to be concerned (and when not to be), and gives you the language to discuss them with a doctor who may never have heard of them in this context.
You are not alone. You are not imagining it. And after reading this, you'll finally understand what your body is doing — and why.
You're Not Imagining It — And You're Not Going Crazy
Why the Strangest Symptoms Are the Loneliest
The classic perimenopause symptoms — hot flashes, irregular periods, insomnia, mood changes — have achieved cultural recognition. They're on every checklist. They're discussed (sometimes even joked about) publicly. When you experience them, you have a framework: "Ah, this is perimenopause."
The obscure symptoms have no such framework.
When you feel electric shocks running through your body, you don't think "hormones." You think "MS" or "nerve damage." When your tongue burns for no reason, you think "cancer" or "allergic reaction." When your skin crawls with no visible cause, you think "parasites" or "psychological."
And because these symptoms are:
Not on any standard perimenopause checklist
Not taught in most medical training
Difficult to describe ("my body vibrates internally" doesn't translate easily to medical language)
Intermittent and unpredictable — appearing and disappearing without pattern
…they create a unique form of isolation. You can't casually mention them at dinner. You can't easily explain them to your partner. And when you describe them to your doctor, the response is often a blank stare, a referral, or — worst of all — the implication that it's anxiety.
This article exists because no woman should have to spend months believing she has a serious disease when what she has is a hormonal transition producing somatic symptoms that medical education hasn't caught up with.
The Medical Term for What You're Experiencing
In clinical research, what you're experiencing falls under what's called the somatic and obscure symptomatology of the menopausal transition — a category of physical symptoms that:
Are driven by neurological, immunological, and autonomic responses to hormonal fluctuation
Don't fit neatly into the standard vasomotor/psychological/urogenital symptom categories
Are vastly underreported in medical literature relative to their prevalence
Are often attributed to other conditions or dismissed as psychosomatic
This isn't a fringe concept. A 2023 systematic review in Maturitas acknowledged that the symptom burden of the menopausal transition extends far beyond the traditionally recognized categories — and called for more research into these "non-classical" manifestations.
Your symptoms have a name. They have a mechanism. And they deserve recognition.
How This Article Is Organized
We've organized every obscure symptom by body system — mirroring how your body actually experiences them. For each symptom, you'll find:
What it feels like (in real women's language)
Why it happens (the hormonal/neurological mechanism)
How common it is (to the extent research tells us)
When to investigate further (the red flag line)
Let's begin.


Why Perimenopause Produces Such Strange Symptoms
Before diving into individual symptoms, understanding why perimenopause can produce such bizarre sensations will help everything else make sense.
Estrogen Receptors — They're Literally Everywhere
This is the foundational fact: estrogen receptors exist in virtually every tissue in your body — brain, nerves, blood vessels, skin, gut, joints, immune cells, sensory organs, oral mucosa, and beyond.
When estrogen was stable, these receptors operated seamlessly in the background. You never noticed them because they were doing their job.
Now that estrogen is fluctuating wildly — spiking, crashing, unpredictable — every tissue with estrogen receptors can produce aberrant signals. That's why the symptoms are so diverse and seemingly unrelated: they're all downstream effects of the same hormonal instability expressing itself through different tissue types.
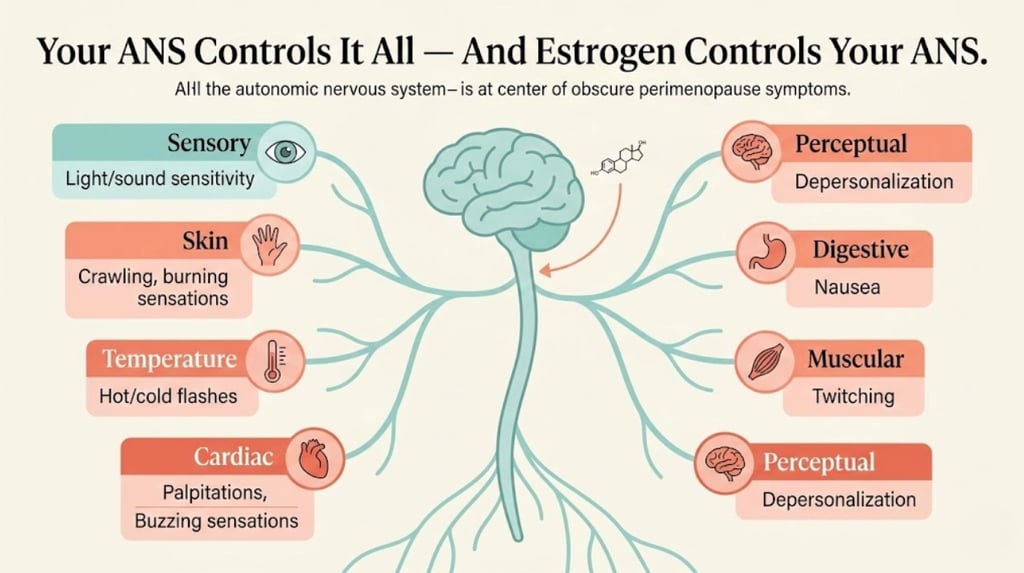
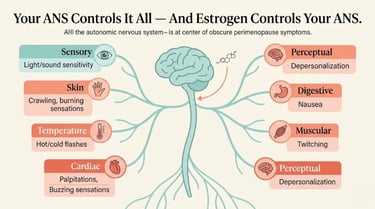
The Nervous System Recalibration
Your autonomic nervous system (ANS) — the system that controls everything you don't consciously control (heart rate, temperature, digestion, blood pressure, sweating, sensory processing) — is profoundly influenced by estrogen.
During perimenopause, your ANS goes through a recalibration — adapting to a new hormonal environment. During this adaptation:
Sensory signals get amplified — things that normally wouldn't register (mild nerve firing, temperature fluctuations, internal organ sensations) become perceptible and sometimes alarming
The fight-or-flight system becomes more reactive — creating physical anxiety symptoms (air hunger, chest sensations, adrenaline surges) without psychological triggers
Thermoregulation malfunctions — not just hot flashes, but cold flashes, internal temperature confusion, and bizarre sweating patterns
Pain processing changes — your brain interprets normal signals as painful or abnormal (central sensitization)
Many of the "weird" symptoms are your nervous system overreacting to normal internal signals because its calibration settings have been disrupted.
Inflammation, Histamine, and Hypersensitivity
Estrogen modulates histamine release and mast cell activation. As estrogen fluctuates:
Histamine levels can surge — causing itching, flushing, hives, skin reactivity, nasal congestion, headaches, and GI disturbance
Mast cells become more reactive — releasing inflammatory mediators that create seemingly random, transient symptoms
The enzyme DAO (diamine oxidase), which breaks down histamine, is estrogen-dependent — so as estrogen drops, histamine clearance may slow
This estrogen-histamine-mast cell axis is one of the most important and least discussed mechanisms behind obscure perimenopause symptoms. It explains allergic-type reactions, skin sensations, and GI symptoms that appear "out of nowhere."
When Your Brain Interprets Hormonal Chaos as Physical Sensation
The brain doesn't just process body signals — it interprets them. And interpretation is shaped by context, including hormonal context.
During perimenopause, your brain may:
Amplify faint signals that it would normally ignore
Misinterpret normal internal activity (nerve firing, muscle contraction, blood flow changes) as something abnormal
Generate sensations in the absence of an external stimulus (phantom smells, internal vibrations, perceived movement)
Lower the threshold for what registers as pain, discomfort, or alarm
This isn't "it's all in your head." It's neurological reality — your brain's sensory processing hardware is being modulated by a changing hormonal environment, and the result is physical sensations that are genuinely felt, even when structurally nothing is wrong.
Neurological and Sensory Symptoms
Electric Shock Sensations
What it feels like:
A sudden, sharp, zapping sensation — like a brief electrical jolt
Often felt in the head, face, arms, or torso
Can precede a hot flash (sometimes called a hot flash "aura")
May occur randomly — sitting at your desk, lying in bed, mid-conversation
Lasts a fraction of a second but is startling and alarming
Why it happens:
Estrogen influences nerve conduction velocity and the sensitivity of peripheral nerve fibers. As estrogen fluctuates, nerves can misfire — producing brief, intense sensations interpreted as electrical shocks. The hypothalamus (your hormonal control center) may also generate these signals during thermoregulatory misfires.
How common: Widely reported in perimenopause communities; under-studied in clinical literature. Not rare.
When to investigate: If shocks are persistent, worsening, or accompanied by weakness, vision changes, or loss of coordination, rule out neurological conditions (MS, neuropathy). In isolation with other perimenopause symptoms, they're almost always hormonal.
Tingling, Numbness, and Pins and Needles (Paresthesia)
What it feels like:
Tingling in hands, feet, fingers, toes, face, or scalp
Pins-and-needles sensation without having been in an awkward position
Numbness or "deadened" feeling in extremities
Sometimes described as "ants walking under the skin"
Why it happens:
Estrogen supports peripheral nerve health and myelin (the insulating sheath around nerves). Fluctuating estrogen can temporarily alter nerve signal transmission. Additionally, changes in blood flow (mediated by estrogen's effect on blood vessels) can create transient ischemic sensations in extremities.
Compounding factors: Vitamin B12 deficiency, low iron, and thyroid dysfunction — all more common in midlife — can worsen paresthesia. These should be tested.
When to investigate: If numbness is persistent, progressive, or unilateral (only one side of the body), neurological evaluation is warranted. Bilateral, intermittent tingling in the context of perimenopause is very commonly hormonal.
Internal Tremors and Vibrating Sensations
What it feels like:
A vibrating or buzzing sensation inside your body — chest, abdomen, limbs
Feels like a cell phone is vibrating inside you
No visible tremor — others can't see it
Often noticed when lying still (especially at night)
Why it happens:
The autonomic nervous system is in a state of heightened reactivity during perimenopause. Internal tremors are thought to result from micro-muscular contractions and autonomic nerve activity that you become aware of because your sensory threshold has lowered. Elevated cortisol and adrenaline — which are more reactive during the transition — can amplify these sensations.
How common: Very commonly reported in perimenopause support groups. Poorly studied formally.
When to investigate: If tremors are visible to others, progressive, or accompanied by other neurological symptoms, evaluation for essential tremor, thyroid dysfunction, or other conditions is appropriate. Internal-only vibrations in perimenopause context are typically benign.
Tinnitus (Ringing or Buzzing in the Ears)
What it feels like:
A persistent or intermittent ringing, buzzing, humming, or hissing in one or both ears
May fluctuate with your cycle or stress levels
Can worsen in quiet environments (especially noticeable at night)
Why it happens:
Estrogen receptors exist in the cochlea (inner ear) and auditory nerve pathways. Estrogen influences blood flow to the inner ear and the sensitivity of auditory neurons. Fluctuating levels can create auditory hypersensitivity and phantom sounds. Additionally, changes in blood pressure and fluid balance during perimenopause may contribute.
Research: A study in Hearing Research found that hormonal fluctuations are associated with changes in auditory function — supporting the estrogen-cochlea connection.
When to investigate: If tinnitus is sudden-onset, unilateral, or accompanied by hearing loss or dizziness, audiological evaluation is important. Bilateral, fluctuating tinnitus that coincides with perimenopause symptoms is likely hormonal.
Dizziness, Vertigo, and Spatial Disorientation
What it feels like:
Lightheadedness — especially when standing up
A sense of the room spinning (true vertigo)
Feeling off-balance or unsteady — "like the ground isn't quite where it should be"
Brief episodes of spatial disorientation — feeling "disconnected" from your physical position
Why it happens:
Multiple mechanisms converge:
Blood pressure regulation changes — estrogen supports vascular tone; fluctuations can cause orthostatic drops
Inner ear sensitivity — estrogen affects vestibular function
Blood sugar instability — insulin sensitivity changes in perimenopause can cause dizzy episodes
Cervicogenic dizziness — increased muscle tension in the neck (common during perimenopause) can affect balance
Anxiety activation — hyperventilation and autonomic reactivity can produce lightheadedness
When to investigate: Persistent vertigo, vertigo with hearing loss, or episodes that cause falls should be evaluated. Brief, positional lightheadedness with other perimenopause symptoms is very commonly hormonal.
Altered Smell and Phantom Odors
What it feels like:
Phantosmia — smelling something that isn't there (smoke, burning, chemicals, perfume)
Hyperosmia — smells seeming much more intense than before
Parosmia — familiar smells seeming wrong or distorted
Your partner's scent may smell different to you
Why it happens:
The olfactory bulb and olfactory processing areas in the brain have estrogen receptors. Estrogen modulates how your brain processes and interprets odor signals. Fluctuating levels can create heightened sensitivity, phantom signals, or distorted interpretation.
How common: More common than recognized. Often dismissed or attributed to anxiety.
When to investigate: Persistent phantosmia (especially burning smells) can rarely be associated with neurological conditions or ENT issues. A brief assessment is reasonable. In perimenopause context, it's usually benign and transient.
Changes in Taste — Metallic, Bitter, or Dulled
What it feels like:
A persistent metallic taste in your mouth
Food tasting different — blander, more bitter, or "off"
Reduced pleasure from foods you used to enjoy
Sometimes described as "pennies in my mouth"
Why it happens:
Estrogen influences taste bud receptor sensitivity and saliva composition. Changes in saliva (reduced flow, altered pH) during perimenopause can alter how taste receptors function. Dry mouth (see oral section below) compounds the effect.
Increased Sensitivity to Light, Sound, or Touch
What it feels like:
Photophobia — bright lights seem more glaring
Phonophobia — sounds that were normal now feel intrusive or overwhelming
Tactile sensitivity — clothing tags, seams, textures that never bothered you now feel irritating
A general sense that your sensory volume has been turned up
Why it happens:
This is central sensitization in action — your brain's sensory processing centers have become more reactive due to hormonal instability. Estrogen modulates sensory gating (the brain's ability to filter out irrelevant stimuli). When estrogen fluctuates, the gating weakens — and more stimuli get through, more intensely.
This is the same mechanism that underlies migraine with aura, which worsens during perimenopause for many women.
Skin and Surface Symptoms
Formication — The Crawling Skin Sensation
What it feels like:
A sensation of insects crawling on or under your skin — with nothing there
Can occur anywhere — face, scalp, arms, legs, torso
Sometimes accompanied by a prickly or itchy quality
Can be maddening — the urge to scratch something that isn't visible
Why it happens:
The term formication (from Latin formica = ant) describes a specific type of tactile hallucination produced by peripheral nerve hypersensitivity. Estrogen supports healthy nerve fiber function in the skin. As levels fluctuate, cutaneous nerve endings become hyperexcitable — generating sensory signals in the absence of external stimulation. Histamine release from mast cells in the skin can compound the sensation.
How common: Reported by a significant minority of perimenopausal women. One of the most distressing obscure symptoms due to its psychological impact.
When to investigate: Persistent formication should prompt a check for B12 deficiency, iron deficiency, thyroid dysfunction, and (rarely) dermatological conditions. If associated with visible skin lesions, dermatological evaluation is appropriate.
Burning Skin — No Rash, No Explanation
What it feels like:
A burning sensation on the skin — as if you have mild sunburn — without any visible change
Often on arms, face, scalp, or upper back
Can be localized or shifting
Sometimes accompanied by skin that feels hot to touch (or feels hot to you but not to others)
Why it happens:
Neuropathic sensitization of cutaneous (skin) nerve fibers. Estrogen withdrawal affects the small fiber nerves in the skin that detect temperature and pain. When these fibers become hyperactive, they produce burning sensations without tissue damage. This is essentially neuropathic pain at the skin level — driven by hormonal change rather than nerve injury.
Itchy Skin (Pruritus) Without Visible Cause
What it feels like:
Intense itching — arms, legs, scalp, torso — without rash, hives, or visible skin changes
Worse at night (when sensory thresholds drop)
May be worse in dry weather or after hot showers
Scratching provides momentary relief but doesn't resolve it
Why it happens:
Three converging mechanisms:
Collagen and moisture loss — declining estrogen reduces skin hydration and collagen, making skin drier and more prone to irritation
Histamine release — estrogen fluctuations can trigger mast cell degranulation, releasing histamine into the skin
Nerve fiber sensitization — cutaneous nerves become more reactive to stimuli that normally wouldn't cause itching
Increased Static Shocks
What it feels like:
Getting shocked more frequently when touching metal objects, other people, or synthetic fabrics
A sense that your body is "more electric" than it used to be
Why it happens:
This one is partly physiological and partly environmental. Drier skin (from estrogen decline) generates more static electricity. Additionally, changes in sweat composition and skin conductivity during perimenopause may alter how your body stores and discharges static charge.
Less scientifically verified — but consistently reported by perimenopausal women in sufficient numbers to warrant inclusion.
Skin That Bruises More Easily
What it feels like:
Bruises appearing from minimal contact — or bruises you can't remember getting
Bruises that take longer to heal
More prominent bruising on arms and legs
Why it happens:
Estrogen supports blood vessel wall integrity and collagen in the vascular system. As estrogen declines, capillary fragility increases — meaning blood vessels in the skin break more easily under minor pressure. Collagen loss also thins the protective tissue around blood vessels.
When to investigate: Easy bruising can also indicate platelet disorders, clotting issues, or vitamin K deficiency. If bruising is excessive or accompanied by other bleeding symptoms (nosebleeds, bleeding gums), a blood count and coagulation screen are warranted.
Changed Body Odor
What it feels like:
Your natural scent has changed — and you notice it
Sweat smells different than it used to
Your partner or close family may notice too
Some women describe a more "pungent" or "sharper" body odor
Deodorant that always worked now seems less effective
Why it happens:
Hormonal changes alter sweat gland activity, particularly the apocrine glands (concentrated in armpits and groin), which produce the protein-rich sweat that bacteria metabolize into body odor. Estrogen and progesterone fluctuations change the composition of this sweat. Additionally, changes in gut microbiome and systemic metabolism during perimenopause can alter the volatile organic compounds your body produces.
New or Worsened Allergic Skin Reactions
What it feels like:
New sensitivities to skincare products, laundry detergent, jewelry, or fabrics
Hives or rashes that appear without clear trigger
Contact dermatitis from products you've used for years
Eczema-like patches appearing for the first time
Why it happens:
The estrogen-histamine-mast cell axis. Fluctuating estrogen can increase mast cell reactivity and histamine release in the skin — lowering the threshold for allergic-type reactions. Your immune system is in a state of relative instability during perimenopause, and skin (your largest organ) often bears the visible evidence.
Oral and Dental Symptoms
Burning Mouth Syndrome (BMS)
What it feels like:
A burning, scalding, or tingling sensation in the mouth — especially the tongue, palate, or lips
No visible sores, ulcers, or redness
May be constant or intermittent
Often worse in the afternoon and evening
Can be accompanied by altered taste and dry mouth
Why it happens:
BMS is significantly more common in perimenopausal and postmenopausal women than in any other population. The mechanism is thought to involve:
Neurological: Estrogen decline affects the trigeminal nerve (the nerve supplying sensation to the mouth and face), causing neuropathic pain
Salivary: Reduced saliva flow changes the oral environment
Mucosal: The oral mucosa (lining) has estrogen receptors and thins with estrogen decline
Research: Multiple studies in Oral Diseases and Menopause journal have documented the strong association between BMS and the menopausal transition. It affects approximately 10–40% of menopausal women — a staggering prevalence for a symptom most women have never heard connected to hormones.
What helps: Some women find relief with HRT (which can restore oral mucosal health), alpha-lipoic acid (modest evidence for BMS), clonazepam rinse (topical, not swallowed), or cognitive behavioral approaches to chronic pain. A dentist or oral medicine specialist with knowledge of hormonal BMS can be helpful.
Dry Mouth (Xerostomia)
What it feels like:
A persistent sense of mouth dryness
Difficulty swallowing dry foods
Increased thirst
Waking at night with a dry mouth
Bad breath despite good oral hygiene
Why it happens:
Estrogen and progesterone influence salivary gland function. As levels decline, saliva production can decrease — and saliva composition (pH, protective proteins) can change. This increases susceptibility to dental cavities, gum disease, and oral discomfort.
Important: Dry mouth is also a side effect of many medications common in midlife (antidepressants, antihistamines, blood pressure medications). Always consider medication as a concurrent cause.
Bleeding Gums and Dental Sensitivity
What it feels like:
Gums that bleed more easily during brushing or flossing
Increased dental sensitivity — hot, cold, or sweet triggers
A sense that your gums are receding or your teeth feel different
More frequent dental infections or slow-healing mouth sores
Why it happens:
Estrogen supports gingival (gum) tissue health and blood flow. Declining estrogen can reduce gum tissue resilience, increase inflammatory response to bacteria, and alter the oral microbiome. This is sometimes called menopausal gingivostomatitis.
Action: Increase dental hygiene vigilance. See your dentist if you notice gum changes. Mention that you're in perimenopause — dentists increasingly recognize hormonal oral changes.
Metallic Taste That Won't Go Away
Covered in the sensory section above — but worth emphasizing here in the oral context. A persistent metallic taste (dysgeusia) without dietary cause is frequently hormonal. It often accompanies dry mouth and can be exacerbated by iron supplements or certain medications.
Musculoskeletal Oddities
"Electric" Pain That Moves Around
What it feels like:
Sharp, shooting, or electric-like pain that appears in one location, then another
Lasts seconds to minutes, then vanishes
Not associated with a specific injury or activity
Can appear in seemingly random locations — shin, forearm, ribcage, hand
Why it happens:
Peripheral nerve sensitization combined with fluctuating estrogen's effect on pain signal modulation. The nerves themselves aren't damaged — they're hypersensitive, firing pain signals at a lower threshold. The migratory nature reflects the systemic (whole-body) nature of hormonal nerve sensitization.
Muscle Twitching and Fasciculations
What it feels like:
Small, visible muscle twitches — often in the eyelid, calf, thigh, or arm
Brief, involuntary contractions that you can see under the skin
May be intermittent or occur in clusters
Why it happens:
Magnesium levels, electrolyte balance, and nerve excitability are all influenced by hormonal changes. Estrogen decline can increase neuromuscular excitability — the tendency of motor neurons to fire without voluntary command. Stress, caffeine, and poor sleep (all common in perimenopause) compound the effect.
What helps: Magnesium glycinate (200–400 mg), adequate hydration, stress management. Muscle twitching in perimenopause is almost always benign — not a sign of ALS or other motor neuron disease (a common fear).
Restless Legs — And Restless Everything
What it feels like:
An irresistible urge to move your legs — especially at rest or in bed
Uncomfortable sensations described as crawling, creeping, aching, or tingling in the legs
Sometimes extends to arms or whole body — a generalized restlessness
Why it happens:
Dopamine pathways (which estrogen modulates) are implicated in restless legs syndrome (RLS). Iron and ferritin levels — often low in perimenopausal women with heavy periods — are also critical. Low ferritin is a well-established risk factor for RLS.
Action: Check ferritin. If below 50 ng/mL, supplementation may help significantly. Target ferritin above 75 ng/mL for RLS symptom improvement (per sleep medicine guidelines).
Feeling "Wrong" in Your Body
What it feels like:
A general sense that something is physically off — but you can't articulate what
Your body feels heavier, stiffer, slower, or unfamiliar
A disconnect between your mental image of your body and how it actually feels
Some women describe it as feeling like they're wearing someone else's body
Why it happens:
This is the intersection of proprioceptive changes (estrogen affects joint and muscle receptors that tell your brain where your body is in space), body composition shifts (weight redistribution, muscle loss, fluid retention), and neurological recalibration (your brain's body map is updating to a changing physical reality).
Thermoregulatory Anomalies Beyond Hot Flashes
Cold Flashes and Sudden Chills
What it feels like:
A sudden, intense cold sensation — shivering, goosebumps, teeth-chattering — without being in a cold environment
Sometimes alternates with hot flashes — hot then cold in rapid succession
Can be accompanied by pale skin and a feeling of internal chill
Why it happens:
The same hypothalamic thermoregulatory dysfunction that causes hot flashes can also trigger inappropriate cooling responses. Your narrowed thermoneutral zone can misfire in either direction — perceiving that you're too hot (hot flash) or too cold (cold flash).
The Electric Jolt Before a Hot Flash (Aura)
What it feels like:
A brief zapping or electrical sensation — often in the head, scalp, or chest — immediately before a hot flash begins
Lasts 1–3 seconds, then the heat wave arrives
Not all women experience this, but those who do report it consistently
Why it happens:
This is thought to be the neural firing of the hypothalamic thermoregulatory trigger — the moment your brain's thermostat decides you need to cool down. The electrical sensation is the signal itself, felt consciously because your nervous system's sensitivity threshold has lowered.
Feeling Like Your Internal Temperature Is "Broken"
What it feels like:
Feeling simultaneously hot and cold — hot skin but internal chill, or cold extremities with a burning core
Temperature confusion — not knowing whether you need a blanket or a fan
Feeling like your body doesn't register temperature correctly anymore
Why it happens:
Your thermoneutral zone has narrowed and destabilized. Your hypothalamus — the brain's thermostat — is receiving contradictory signals from estrogen-sensitive pathways, resulting in mixed messages about your actual temperature and the appropriate response.
Excessive Sweating Without Heat Triggers
What it feels like:
Sweating at rest — palms, feet, underarms, back — without being hot or exerting yourself
Night sweats without hot flashes — waking damp without the classic heat wave
Sweating during mild activity that never made you sweat before
Why it happens:
Autonomic nervous system dysregulation affects the eccrine sweat glands (your thermoregulatory sweat glands, distributed across the body). The threshold for sweat activation lowers — so your body sweats at temperatures and activity levels that previously wouldn't trigger it.
Gastrointestinal and Systemic Oddities
Nausea That Comes and Goes Without Reason
What it feels like:
Waves of nausea — sometimes reminiscent of early pregnancy
Not related to food, illness, or motion
Can be triggered by hormonal fluctuations — often before or during a period
May be accompanied by loss of appetite or a general "queasy" feeling
Why it happens:
Estrogen influences gastric motility, acid production, and the gut-brain axis. Hormonal surges — particularly estrogen spikes — can trigger nausea through the same mechanisms that cause morning sickness in pregnancy (same hormone, less extreme fluctuation).
Feeling Hungover Without Drinking
What it feels like:
Waking up feeling groggy, headachy, dehydrated, and brain-fogged — as if you drank heavily the night before
No alcohol was consumed
Sometimes accompanied by mild nausea and extreme fatigue
Often occurs on mornings after night sweats or poor sleep
Why it happens:
The "perimenopause hangover" is likely caused by a combination of: cortisol surges during the night (disrupted HPA axis), dehydration from night sweats, sleep architecture disruption (less deep sleep), and inflammatory metabolites from the hormonal cascade. Your body is literally processing the aftermath of a hormonal event.
Reduced Alcohol and Caffeine Tolerance
What it feels like:
One glass of wine now affects you like three used to
Coffee makes you jittery, anxious, or gives you palpitations — even at amounts you used to tolerate
Alcohol causes worse sleep, more hot flashes, and more intense hangovers than before
You may develop new reactions to alcohol — flushing, headaches, or GI upset
Why it happens:
Multiple converging mechanisms:
Liver enzyme changes — estrogen influences how your liver metabolizes alcohol and caffeine. Fluctuating levels alter enzyme efficiency
Increased inflammatory sensitivity — alcohol is pro-inflammatory; your body's inflammatory set-point has shifted upward
Histamine — alcohol (especially red wine, beer, and champagne) is high in histamine. With reduced DAO activity during perimenopause, histamine clearance is impaired
Autonomic reactivity — caffeine stimulates a nervous system that's already hyperactivated
Sleep vulnerability — even moderate alcohol further disrupts the already-compromised sleep architecture of perimenopause
Histamine Reactions and New Food Sensitivities
What it feels like:
New reactions to foods you've always eaten — flushing, headaches, hives, bloating, nasal congestion
Reactions to high-histamine foods: aged cheese, wine, fermented foods, chocolate, tomatoes, cured meats
Symptoms that seem "allergic" but allergy testing comes back negative
Why it happens:
The estrogen-histamine-DAO axis. Estrogen stimulates both histamine production AND the production of DAO (the enzyme that clears histamine). As estrogen fluctuates, this system becomes unbalanced — sometimes too much histamine is produced, sometimes too little is cleared. The result: histamine intolerance symptoms that look like allergies but are hormonally driven.
Evidence level: This area is supported by growing but still limited clinical evidence. The mechanism is biologically plausible, widely observed clinically, and increasingly recognized by functional medicine practitioners. Large-scale studies are needed.
Random Blood Sugar Crashes
What it feels like:
Sudden weakness, shakiness, brain fog, irritability — especially between meals
Feeling like you must eat immediately or you'll collapse
Episodes that resolve quickly after eating carbohydrates
Why it happens:
Declining estrogen reduces insulin sensitivity — your cells respond less effectively to insulin, causing more dramatic blood sugar swings. This can produce reactive hypoglycemia — blood sugar dropping too quickly after an insulin spike, especially if meals are carb-heavy or irregularly timed.
Cardiac and Respiratory Sensations
The "Buzzing Chest" — Vibrations You Can't Explain
What it feels like:
A vibrating or buzzing sensation in your chest — not a heartbeat, not a flutter, but a vibration
May be felt in the sternum area or behind the left breast
Often more noticeable when lying down or at rest
Alarming because it's in the chest — immediately triggers cardiac worry
Why it happens:
Likely a combination of autonomic nerve activity in the chest wall, intercostal muscle micro-contractions (small muscles between the ribs), and heightened interoception (your brain's increased awareness of internal body sensations). Not a cardiac symptom — but understandably frightening.
When to investigate: Any chest symptom warrants at least a basic ECG and cardiovascular check to rule out arrhythmia. Once cardiac causes are excluded, the vibrating sensation can be attributed to neuromuscular/autonomic origin.
Air Hunger — Feeling Like You Can't Take a Full Breath
What it feels like:
A sense that you can't get a satisfying breath — you keep trying to take a deep breath and it doesn't "land"
Sighing frequently to try to fill your lungs
No wheeze, no cough, no congestion — just an unsatisfied feeling when breathing
Often worse during periods of anxiety or when focused on it
Why it happens:
Air hunger (dyspnea) without respiratory pathology is a classic autonomic nervous system symptom. During perimenopause:
Elevated cortisol and adrenaline increase respiratory rate — causing subtle hyperventilation
Hyperventilation lowers CO2 levels — which paradoxically makes you feel like you're not getting enough air
Estrogen receptors in the brainstem respiratory center are being stimulated inconsistently
Anxiety amplifies the sensation — creating a feedback loop
What helps: Slow, extended exhale breathing (in for 4, out for 7–8). This resets CO2 levels and calms the autonomic nervous system. Nasal breathing. Reassurance that your lungs are structurally fine.
Heart "Flutters" That Aren't Classic Palpitations
What it feels like:
Not the typical "racing heart" — more like a quivering, fluttering, or rippling sensation in the chest
May feel like your heart is doing something different but you can't quite describe it
Sometimes accompanied by a brief wave of anxiety or adrenaline
Why it happens:
These may represent ectopic beats (premature atrial or ventricular contractions — very common and usually benign), changes in heart rhythm variability (HRV shifts during perimenopause), or simply heightened interoceptive awareness of normal cardiac activity.
Psychological and Cognitive Oddities
Depersonalization — Feeling Disconnected from Yourself
What it feels like:
A sensation of observing yourself from outside — as if you're watching your life through glass
Feeling emotionally numb or detached from reality
The world looking slightly unreal, dreamlike, or two-dimensional
Brief episodes that come and go — often during periods of high stress or fatigue
Why it happens:
Depersonalization is a dissociative response that can be triggered by hormonal instability, sleep deprivation, anxiety, and autonomic nervous system activation — all of which converge during perimenopause. Estrogen influences serotonin and GABA — neurotransmitters involved in your sense of self and reality grounding.
Important reassurance: Depersonalization during perimenopause is transient and benign. It does not mean you're developing a dissociative disorder. It's a stress response — and your nervous system is under significant hormonal stress.
Intrusive Thoughts That Aren't "You"
What it feels like:
Sudden, unwanted, disturbing thoughts that pop into your mind — about harm, death, disaster, or taboo subjects
They feel foreign — not aligned with your values or personality
They create intense guilt, shame, or anxiety — "Why am I thinking this?"
They're ego-dystonic — meaning they distress you because they DON'T represent who you are
Why it happens:
Intrusive thoughts are a feature of anxiety — and perimenopausal anxiety has unique neurochemical drivers. Fluctuating estrogen affects serotonin (which normally helps the brain filter and dismiss intrusive thoughts) and the amygdala (which becomes more reactive). With less serotonin-mediated filtering and a more reactive fear center, intrusive thoughts that would normally be silently discarded become conscious and alarming.
Critical distinction: Intrusive thoughts are NOT intentions. They don't mean you want to act on them. They're misfired anxiety signals — and they're extremely common, especially during hormonal transitions. If they're causing significant distress, CBT (cognitive behavioral therapy) is highly effective.
The "Wrong Speed" Feeling
What it feels like:
A sense that life is moving too fast — or that time has an unfamiliar quality
Feeling behind, overwhelmed, or unable to keep up — even when your schedule is normal
A disconnect between your internal rhythm and external reality
Why it happens:
Time perception and processing speed are influenced by dopamine (which estrogen modulates). Changes in dopamine signaling can alter how quickly or slowly time seems to pass. Combined with brain fog, reduced processing speed, and the cognitive load of managing a hormonal transition, the subjective experience is that life's pace has changed — when really, your brain's processing speed has.
Emotional Synesthesia — Feeling Emotions Physically in Your Body
What it feels like:
Experiencing emotions as literal physical sensations — anxiety as chest pressure, sadness as physical heaviness, anger as heat
Emotions feel more physical than they used to
Your body and your emotions feel less separate than before
Why it happens:
Estrogen modulates the insula — the brain region that integrates emotional processing with bodily awareness. During perimenopause, the connection between emotional states and physical sensation can become amplified — making emotions feel more bodily and body sensations feel more emotional.
What Women Actually Experience — The Symptoms That Made Them Think They Were Losing It
"I Thought I Had a Neurological Disease"
"At 45, I started getting electric shock sensations in my head and arms. Then my hands went tingly. Then I noticed my calves twitching at night. I was SURE I had MS. I demanded an MRI. It was clean. I demanded nerve conduction studies. Normal. I saw a neurologist who ran every test he could think of and found absolutely nothing wrong. He shrugged and said 'it's probably stress.' It wasn't until I mentioned it in a perimenopause Facebook group that twenty women said 'YES. Exactly this. It's hormonal.' I cried. Not because I was sad — because I'd spent six months terrified, and the answer had been my hormones all along."
"I Was Convinced Something Was Seriously Wrong"
"My tongue started burning at 47. Burning — like I'd eaten something scalding. But I hadn't. It got worse throughout the day, every day. I went to my dentist. Nothing visible. My GP. Nothing on blood tests. An ENT. Nothing. An oral medicine specialist finally said: 'This is burning mouth syndrome. It's very common in women your age. It's connected to hormonal changes.' I'd seen FOUR professionals before hearing the word 'hormones.' Four."
"The Relief of Finding Out It Was Hormonal"
"I had the crawling skin, the electric shocks, the weird nausea, the changed body odor, and a vibrating sensation in my chest. I was googling symptoms at 2 a.m., convinced I had fibromyalgia, a thyroid tumor, and a cardiac condition — simultaneously. When a menopause specialist looked at my full list and said: 'Every single one of these is a known somatic manifestation of perimenopause. Let me explain why,' I felt my whole body relax. Not because the symptoms went away — they were still there. But because I finally had a FRAMEWORK. A reason. A name. And that changed everything."
"My Doctor Had Never Heard of This Symptom in Perimenopause"
"When I told my GP about the burning skin sensation — no rash, no redness, just a feeling of being mildly sunburned all the time — she looked at me like I was speaking another language. She ran some dermatology tests, checked my B12, and said she couldn't explain it. When I showed her an article about cutaneous nerve sensitization during estrogen decline, she read it, paused, and said: 'I've honestly never come across this. Thank you for bringing it in.' She wasn't dismissive — she just didn't know. That's the problem. The information exists in research papers. It just hasn't reached clinical practice."
What Science Says — The Somatic and Obscure Symptomatology of Perimenopause
Why These Symptoms Are Under-Researched
The gap between what women experience and what medical literature covers is wide — and there are structural reasons:
Research funding priorities favor conditions with high mortality (cancer, heart disease) over quality-of-life symptoms
Menopause research has historically focused on the "big three" — vasomotor symptoms, bone health, and cardiovascular risk
Somatic symptoms are harder to measure objectively — they're subjective, intermittent, and variable
Gender bias in medicine has historically framed unexplained physical symptoms in women as psychological
Specialist silos mean that a neurologist studying tinnitus, a dermatologist studying formication, and a gastroenterologist studying nausea don't share a conference room — and may not realize they're seeing different expressions of the same hormonal transition
The Autonomic Nervous System — The Hidden Control Center
The autonomic nervous system (ANS) is the master controller of involuntary body functions — and it's profoundly estrogen-sensitive.
During perimenopause, ANS dysregulation produces a constellation of symptoms that are hard to categorize because they affect every system the ANS controls:
Understanding that these are all ANS-mediated — and that the ANS is estrogen-regulated — transforms a bewildering list of random symptoms into a coherent pattern with a single driver.
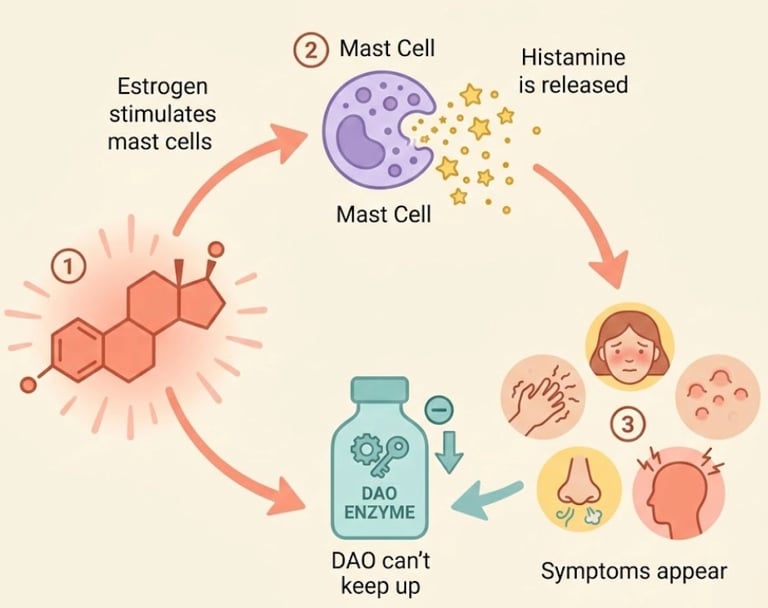
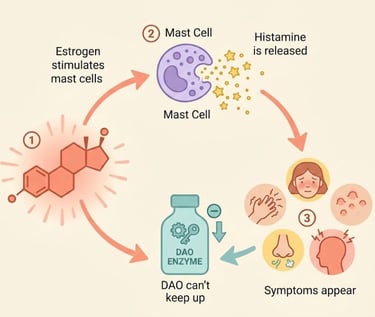
Estrogen, Histamine, and Mast Cell Activation
The estrogen-histamine connection deserves its own section because it explains a cluster of symptoms that are otherwise inexplicable:
The mechanism:
Estrogen stimulates mast cells to release histamine
Histamine stimulates the ovaries to produce more estrogen
This creates a bidirectional amplification loop
Meanwhile, DAO (the enzyme that clears histamine) is estrogen-dependent — so when estrogen drops, histamine clearance slows
During perimenopause:
Estrogen spikes → massive histamine release → flushing, itching, hives, headaches, nasal congestion, GI upset
Estrogen crashes → DAO drops → histamine accumulates → same symptoms from a different mechanism
Symptoms explained by this axis:
Itchy skin without rash
New food sensitivities
Flushing unrelated to hot flashes
Worsened allergies
Hives or urticaria
Nasal congestion
Headaches (histamine is a potent vasodilator in the brain)
Evidence level: Biologically well-established at the cellular level. Clinical application to perimenopause is growing but not yet mainstream. Functional medicine and allergy specialists are increasingly recognizing this connection.
Central Sensitization — When the Volume Gets Turned Up
Central sensitization is a neurological state where the central nervous system amplifies sensory signals — making normal inputs feel abnormal, uncomfortable, or painful.
During perimenopause, central sensitization can develop due to:
Fluctuating serotonin (which helps regulate sensory input)
Reduced endorphin production (estrogen supports endorphin pathways)
Chronic stress/cortisol (which sensitizes the nervous system)
Sleep deprivation (which lowers pain and sensory thresholds)
Central sensitization explains why:
Your skin hurts when nothing is touching it
Normal lights seem too bright
Normal sounds seem too loud
Your body feels pain at a lower threshold than before
Internal sensations (heartbeat, digestion, nerve firing) become consciously perceptible when they were previously filtered out
This is not psychosomatic. It's neurophysiological — and it's reversible as hormones stabilize or with targeted interventions.
What's Established vs. What's Emerging vs. What's Anecdotal
Scientifically established:
Estrogen receptors exist throughout the nervous system, skin, oral mucosa, gut, cardiovascular system, and sensory organs
Autonomic nervous system function is estrogen-dependent
Burning mouth syndrome is strongly associated with the menopausal transition
Musculoskeletal symptoms (including atypical pain patterns) affect 50–60% of transitioning women
Central sensitization can be hormonally modulated
Emerging (supported by growing evidence):
The estrogen-histamine-mast cell axis as a driver of allergic/inflammatory symptoms
Formication, electric shocks, and paresthesia as neurologically-mediated perimenopausal symptoms
Tinnitus and vestibular changes linked to estrogen fluctuations
Changes in pain perception thresholds during the menopausal transition
Interoceptive amplification (heightened awareness of internal body signals) as a feature of hormonal transition
Anecdotal but consistently reported:
Increased static shocks
Changed body odor
Internal vibrating/buzzing sensations
"Hangover" feeling without alcohol
Phantom smells
Temperature "confusion" (simultaneously hot and cold)
The "wrong speed" cognitive sensation
These anecdotal symptoms are reported with such consistency and specificity across diverse populations of perimenopausal women that they almost certainly have biological underpinnings — but they haven't yet received formal research attention.
This article is for educational purposes and does not replace medical advice. Many of these symptoms, while commonly hormonal, can also have other causes. New, persistent, or concerning symptoms should be evaluated by a healthcare provider to rule out other conditions.
When Weird Symptoms Need Medical Attention
The Difference Between "Weird but Hormonal" and "Weird and Needs Investigation"
Most obscure perimenopause symptoms are benign, temporary, and hormonal. But because they overlap with symptoms of other conditions, here's how to differentiate:
Likely hormonal if:
☐ Appeared during your 40s–50s alongside other perimenopause symptoms
☐ Intermittent — comes and goes rather than being constant and worsening
☐ Bilateral or diffuse — affects both sides, or moves around
☐ Correlates with your cycle, stress level, or sleep quality
☐ Standard tests (blood work, imaging) come back normal
☐ Fits patterns described by other perimenopausal women
Warrants investigation if:
☐ Unilateral — affects only one side of the body
☐ Progressive — steadily worsening over weeks/months
☐ Associated with neurological deficits (weakness, vision changes, loss of coordination)
☐ Accompanied by unexplained weight loss, fever, or night sweats (different from perimenopause sweats)
☐ New and sudden-onset with no prior perimenopausal context
☐ Causes significant functional impairment
Red Flags That Warrant Urgent Evaluation
🚩 Sudden-onset unilateral weakness or numbness — stroke risk assessment
🚩 Sudden severe headache ("worst headache of my life") — requires emergency evaluation
🚩 Visual disturbances (loss of vision, double vision, visual field changes) — neurological or ophthalmological evaluation
🚩 Chest pain with exertion — cardiac evaluation
🚩 Persistent unilateral tinnitus with hearing loss — audiological/neurological evaluation
🚩 Rapidly progressive symptoms of any kind — specialist assessment
🚩 Seizure-like episodes — neurological evaluation
🚩 Unexplained bleeding from any site — appropriate investigation
The Tests Worth Running to Rule Out Other Causes
If you're experiencing multiple obscure symptoms, these baseline investigations help exclude non-hormonal causes:
What Actually Helps
HRT — Does It Help the Weird Symptoms Too?
Short answer: often, yes — sometimes dramatically.
HRT restores systemic estrogen — which means every tissue with estrogen receptors begins to function more normally. This includes:
Nerves → reduced electric shocks, tingling, burning skin
Oral mucosa → improved burning mouth syndrome
Skin → reduced itching, formication, dryness
ANS → improved temperature regulation, reduced palpitations, better sensory gating
Brain → reduced central sensitization, better sensory filtering, improved interoceptive calibration
Many women with obscure symptoms report that HRT resolved symptoms they didn't even start HRT for — the weird symptoms improved as a "bonus" alongside the classic symptoms they were primarily treating.
Important nuance: Not all obscure symptoms respond equally to HRT. Some — particularly those involving central sensitization or histamine — may need additional targeted approaches.
Nervous System Regulation Strategies
Since many obscure symptoms stem from ANS dysregulation, strategies that calm and reset the nervous system can be remarkably effective:
Vagus nerve stimulation techniques: Extended exhale breathing (in for 4, out for 7-8), cold water on the face (dive reflex), humming, gargling
Polyvagal-informed practices: Gentle yoga, tai chi, walking in nature — activities that activate the ventral vagal (calm and connected) state
Progressive muscle relaxation — systematically tensing and releasing muscle groups to reduce background muscle tension and nerve excitability
Somatic experiencing therapy — a body-based therapeutic approach specifically designed for nervous system regulation
Limiting nervous system stimulants — caffeine, alcohol, screens before bed, high-intensity exercise close to bedtime
Anti-Histamine Approaches
For symptoms that align with the histamine-mast cell axis:
Low-histamine diet trial (2–4 weeks) — reducing aged cheeses, wine, fermented foods, processed meats, tomatoes, chocolate, vinegar. If symptoms improve, histamine intolerance is likely contributing
DAO enzyme supplementation — taken before meals, may help break down dietary histamine (emerging evidence)
Quercetin — a natural mast cell stabilizer. Found in apples, onions, capers, and available as a supplement. Modest evidence
Vitamin C — supports DAO production and acts as a natural antihistamine
Over-the-counter antihistamines — cetirizine or loratadine may help if histamine symptoms are prominent. Discuss with your provider
Avoiding histamine triggers — alcohol, heat, intense exercise, and stress all promote histamine release
The Role of Magnesium, B Vitamins, and Omega-3s
These three nutrients come up repeatedly because they support the neurological, immunological, and inflammatory systems that drive obscure symptoms:
🔎 Recommended Tools and Resources
This article may contain affiliate links. We only recommend products we've researched and believe may be genuinely useful. Affiliate commissions help support this site at no extra cost to you.
1. "The Menopause Manifesto" by Dr. Jen Gunter
Best for: Comprehensive, evidence-based understanding of all menopausal symptoms — including lesser-known ones
Why it helps here: Dr. Gunter covers neurological and somatic symptoms with scientific rigor. Excellent for validating the symptoms your doctor may not recognize
2. Magnesium Glycinate (200–400 mg)
Best for: Muscle twitching, restless legs, nerve excitability, sleep, anxiety — broad nervous system support
Why it helps here: Magnesium deficiency is common in midlife and exacerbates many somatic symptoms. Glycinate form is gentle and well-absorbed
Evidence level: Modest but positive for multiple relevant symptoms. Low risk
3. Omega-3 Fish Oil (High EPA/DHA)
Best for: Systemic anti-inflammatory support — nerves, brain, joints, skin
Why it helps here: EPA/DHA reduce the inflammatory cytokines that drive many somatic perimenopause symptoms. Support nerve myelin health
4. DAO Enzyme Supplement (for histamine support)
Best for: Women experiencing histamine-related symptoms — flushing, hives, food sensitivities, itching
Why it helps here: Supplemental DAO enzyme helps break down histamine from food, reducing histamine load in women whose natural DAO production has been affected by estrogen fluctuations
Evidence level: Emerging — biologically plausible, limited clinical trials
Important: Not a substitute for investigation of true allergy or mast cell disorders. Best used as a trial alongside dietary histamine reduction
YMYL disclosure: No supplement or practice replaces medical evaluation for new or persistent symptoms. These tools are supportive aids. Histamine-related symptoms should be discussed with a healthcare provider, especially if severe. Individual results vary.
How to Talk About Symptoms Your Doctor Has Never Heard Of
What to Say — Without Sounding "Crazy"
The fear of being dismissed is real — and it stops many women from raising obscure symptoms. Here's how to frame them:
Opening:
"I'm experiencing some physical symptoms that I've researched and believe may be connected to perimenopause — specifically, somatic symptoms related to autonomic nervous system changes during the hormonal transition. I'd like to discuss them and rule out other causes."
Why this works: You've immediately:
Used medical language ("somatic symptoms," "autonomic nervous system")
Demonstrated research ("I've researched")
Shown reasonableness ("rule out other causes")
Positioned yourself as an informed patient, not an anxious Googler
Framing Obscure Symptoms in Medical Language
Using the correct medical terms signals to your doctor that you've done your research — and makes it harder to dismiss your symptoms as vague anxiety.
When to Seek a Specialist
Menopause specialist (NAMS-certified) — for the hormonal perspective and HRT discussion
Neurologist — if neurological symptoms are prominent and need ruling out
Allergist/immunologist — if histamine-related symptoms are dominant
Functional medicine practitioner — for an integrative approach to somatic symptoms
Oral medicine specialist — for burning mouth syndrome specifically
The Complete Obscure Symptom Checklist
Check every symptom you've experienced in the past 6 months:
Neurological & Sensory:
☐ Electric shock sensations
☐ Tingling or pins and needles (paresthesia)
☐ Internal tremors or vibrating
☐ Tinnitus (ringing/buzzing in ears)
☐ Dizziness or vertigo
☐ Phantom smells
☐ Changed or metallic taste
☐ Increased sensitivity to light, sound, or touch
Skin & Surface:
☐ Crawling skin sensation (formication)
☐ Burning skin without rash
☐ Itchy skin without visible cause
☐ More static shocks
☐ Easy bruising
☐ Changed body odor
☐ New allergic skin reactions
Oral & Dental:
☐ Burning mouth/tongue
☐ Dry mouth
☐ Bleeding gums or dental sensitivity
Musculoskeletal:
☐ Migratory "electric" pain
☐ Muscle twitching
☐ Restless legs
☐ Feeling "wrong" in your body
Temperature:
☐ Cold flashes
☐ Electric jolt before hot flash
☐ Internal temperature confusion
☐ Sweating without heat triggers
Gastrointestinal & Systemic:
☐ Random nausea
☐ "Hangover" feeling without drinking
☐ Reduced alcohol/caffeine tolerance
☐ New food sensitivities/histamine reactions
☐ Blood sugar crashes
Cardiac & Respiratory:
☐ Chest buzzing/vibrating
☐ Air hunger
☐ Heart flutters (non-classic)
Psychological & Cognitive:
☐ Depersonalization episodes
☐ Intrusive thoughts
☐ "Wrong speed" feeling
☐ Emotions felt as physical sensations
Your total: ___ / 34
If you checked 5 or more, and you're between 40 and 55 with other perimenopause indicators, these symptoms are very likely connected to your hormonal transition. You're not crazy. You're not sick. Your nervous system is recalibrating.
You're Not Crazy — Your Nervous System Is Recalibrating
If you've read this entire article — and recognized yourself in symptom after symptom — here's what we hope you feel:
Validation. These symptoms are real. They have names. They have mechanisms. They have biological explanations rooted in receptor biology, neuroscience, and immunology. They are not invented, imagined, or exaggerated.
Relief. You don't have MS. You don't have cancer. You don't have a neurological disease. You have a hormonal transition that affects a far wider range of body systems than anyone ever told you it would.
Connection. Millions of women are experiencing these same symptoms right now — and most of them, like you, thought they were alone. The silence around obscure perimenopause symptoms is not a reflection of their rarity. It's a reflection of a medical system that hasn't caught up.
Empowerment. You now have the language, the science, and the framework to talk about these symptoms — with your doctor, your partner, yourself. You can advocate. You can request. You can insist.
Your body isn't betraying you. It's going through the most significant hormonal recalibration since puberty. Every strange sensation is your nervous system adapting to a new reality. It's messy. It's confusing. It's sometimes frightening.
But it is temporary. And you are not alone.
FAQ — Weird Perimenopause Symptoms
Q: Can perimenopause cause electric shock sensations?
A: Yes. Electric shock sensations are a recognized somatic symptom of perimenopause, caused by estrogen's effect on nerve conduction and the sensitivity of peripheral nerve fibers. They're often brief, startling, and may precede hot flashes.
Q: Is burning mouth syndrome related to perimenopause?
A: Yes. Burning mouth syndrome is significantly more common in perimenopausal and postmenopausal women. It's linked to estrogen's influence on the trigeminal nerve, oral mucosa, and salivary function. It affects approximately 10–40% of menopausal women.
Q: Can perimenopause cause skin crawling sensations?
A: Yes. This sensation — called formication — is caused by peripheral nerve hypersensitivity due to estrogen fluctuations. Cutaneous nerve endings become hyperexcitable, generating sensory signals without external stimulation. Histamine release can compound it.
Q: Why am I suddenly sensitive to histamine during perimenopause?
A: Estrogen modulates both histamine production and DAO (the enzyme that clears histamine). During perimenopause, this system becomes unbalanced — leading to histamine accumulation and symptoms like itching, flushing, food reactions, and headaches.
Q: Can perimenopause cause tinnitus?
A: Yes. Estrogen receptors exist in the cochlea and auditory pathways. Fluctuating estrogen can affect inner ear blood flow and auditory nerve sensitivity, producing ringing, buzzing, or humming sounds. Bilateral, fluctuating tinnitus during perimenopause is likely hormonal.
Q: Are these weird symptoms permanent?
A: For most women, no. Obscure somatic symptoms are driven by hormonal instability — the fluctuations of perimenopause. Once hormones stabilize after menopause (or with HRT), most symptoms improve significantly. They reflect a nervous system in transition, not permanent damage.
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References
Perimenopause Compass
Contact
hello@perimenopausecompass.com
© 2026 All rights reserved.