Perimenopause Joint Pain: Is It Hormonal?
Perimenopause joint pain is real — and yes, it's often hormonal. Understand why your joints hurt, what estrogen has to do with it, and what actually helps. Clear answers inside.
EDUCATIONAL
Clara A.
2/28/202621 min read
You wake up and your hands are stiff. Not dramatically — but noticeably. It takes a few minutes of opening and closing your fists before they feel normal. Your knees ache when you stand up from a chair. Your hips are sore in the morning. Your shoulders feel like they belong to someone twenty years older.
You're 44. Or 47. Or 50. And you're thinking: is this arthritis? Is this just aging? Am I falling apart?
You might have seen your GP. Maybe you had blood tests. Maybe the results came back normal — no rheumatoid factor, no inflammatory markers, no autoimmune antibodies. Maybe your doctor said "everything looks fine" and you left feeling confused, because your joints definitely do NOT feel fine.
Here's the answer nobody gave you: yes, your joint pain is very likely hormonal. And no, you're not imagining it.
Perimenopause joint pain is one of the most common — and most underrecognized — symptoms of the hormonal transition. It affects an estimated 50–60% of women during perimenopause and early postmenopause. Yet it rarely appears on the "classic symptoms" lists that women are given. It's not hot flashes. It's not missed periods. So it gets missed.
This article explains exactly why your joints hurt, what estrogen has to do with it, how to tell the difference between hormonal joint pain and conditions like arthritis, and what actually helps — from medical treatments to practical strategies that real women have found effective.
The Short Answer — Yes, It Very Likely Is
Why This Symptom Stays Hidden in Plain Sight
Joint pain is one of perimenopause's best-kept secrets — not because it's rare, but because:
It's not on the "menopause checklist." When women think perimenopause, they think hot flashes, irregular periods, mood swings. Joint pain doesn't make the mental shortlist — so they don't connect it.
It mimics other conditions. Joint pain in a 45-year-old woman looks like arthritis, repetitive strain, or "just getting older." Without the hormonal lens, the hormonal cause is invisible.
Doctors don't ask about it. Most GPs and even gynecologists don't routinely ask perimenopausal women about their joints. And most rheumatologists don't ask about menstrual cycle changes.
Blood tests come back "normal." Standard autoimmune and inflammatory markers (RF, anti-CCP, CRP, ESR) are typically negative in hormonal joint pain — which leads to false reassurance or diagnostic dead ends.
Women minimize it. "It's just stiffness." "I must be sleeping wrong." "I'm probably not exercising enough." The pain is real, but the cultural tendency to dismiss women's pain — compounded by self-dismissal — keeps it invisible.
The result: millions of women are experiencing hormonal joint pain right now and attributing it to aging, arthritis, or bad luck — when the cause is a hormonal shift that is both explainable and treatable.
The Specialist Merry-Go-Round Nobody Warns You About
One of the most frustrating aspects of perimenopausal joint pain is what many women call the specialist merry-go-round:
You see your GP → told it's "wear and tear" or prescribed ibuprofen
You're referred to a rheumatologist → full autoimmune panel comes back negative → "Good news, no arthritis"
You see a physiotherapist → given exercises for "general stiffness"
You return to your GP → possibly referred for imaging → X-rays show "minor degenerative changes" (which are normal for your age)
Nobody mentions hormones.
Each specialist sees their organ system. Nobody sees the whole woman going through a hormonal transition. This fragmented care model is why so many women suffer unnecessarily — and why understanding the hormonal connection yourself can be genuinely life-changing.
What Perimenopause Joint Pain Actually Feels Like
This isn't textbook arthritis pain. Perimenopause joint pain has its own signature — and recognizing it is the first step toward understanding it.
Morning Stiffness That Takes Longer to Ease
The most commonly reported pattern:
You wake up and your joints feel rigid, tight, or "locked"
It takes 10–30 minutes of gentle movement before they loosen up
This is worse than anything you experienced in your 30s
It's particularly noticeable in your hands, fingers, and hips.
This morning stiffness is often the very first musculoskeletal sign of perimenopause — appearing before hot flashes, before significant cycle changes, sometimes before women have any idea the transition has begun.
Aching Hands, Hips, Knees, and Shoulders
The ache is distinctive:
A dull, deep soreness rather than sharp pain
Feels like your joints are slightly swollen — even if they don't look it
Worse after inactivity (sitting for long periods, sleeping)
Improves with gentle movement but may worsen with high-impact activity
Can affect multiple joints — unlike an injury, which is usually localized
The intensity fluctuates — some days manageable, some days distracting.
Pain That Moves Around
One of the hallmarks that distinguishes hormonal joint pain from structural conditions:
One week your knees ache. The next week it's your wrists. Then your hips.
The migratory nature of the pain confuses both women and their doctors
This pattern reflects the systemic nature of hormonal change — estrogen receptors exist in every joint, and fluctuating levels can affect different joints at different times.
The "Overnight Aging" Sensation
Women describe this in strikingly consistent language:
"I feel like I aged 20 years overnight"
"My body feels like it belongs to my mother"
"I used to jump out of bed. Now I creak"
"Getting up from the floor takes strategy and planning".
This sensation is not aging. It's hormonal withdrawal affecting joint tissues that have relied on estrogen for decades. The difference matters — because aging is irreversible, but hormonal joint pain is often highly responsive to treatment.
When It's Worse — And When It Eases
Many women notice patterns:
Worse:
In the morning — after hours of immobility
During cold or damp weather (estrogen-depleted joints may be more weather-sensitive)
Before or during your period (when estrogen drops in the cycle)
During periods of high stress (cortisol amplifies inflammation)
After intense or high-impact exercise
On days when you're sleep-deprived
Better:
After gentle movement (walking, stretching, yoga)
In warm environments (warmth improves blood flow and lubrication)
Mid-cycle — when estrogen is typically higher (in women still cycling)
During periods of good sleep and low stress
Some women report improvement with anti-inflammatory foods.
If your joint pain follows a cyclical pattern — worsening and improving with your menstrual cycle — that's one of the strongest indicators that hormones are driving it.
What Women Actually Experience
"I Thought I Had Arthritis at 44"
"My fingers started aching at 44. Not dramatically — more like a constant low-level soreness, especially in the mornings. I couldn't open jars as easily. My wedding ring felt tight by afternoon. I was convinced I had rheumatoid arthritis — my grandmother had it, and this felt like the beginning. My GP ordered blood tests: RF, anti-CCP, CRP, ESR. All normal. The X-rays showed nothing. He said it was probably 'wear and tear' and suggested glucosamine. I spent a year rubbing my aching hands with worry and gel. Nobody mentioned hormones. Not once."
"My Rheumatologist Couldn't Find Anything Wrong"
"At 46, the pain spread to my knees, hips, and shoulders. I was struggling to climb stairs without holding the railing. My rheumatologist did a thorough workup — blood tests, X-rays, ultrasound of my hands. She was excellent. And she found absolutely nothing wrong. 'Your joints are structurally healthy,' she said. 'I can't explain your pain.' I left her office validated that it wasn't autoimmune — but completely without answers. It was a perimenopause support group online that finally connected the dots. Six other women described my exact symptoms. Estrogen was the missing variable nobody was testing for — because nobody thought to ask."
"Nobody Connected My Joint Pain to My Hormones"
"What makes me angry isn't that I had joint pain. It's that I saw FOUR healthcare providers over two years, described all my symptoms — including irregular periods, insomnia, and brain fog — and not one of them said: 'These could all be connected to perimenopause.' They treated every symptom as a separate problem. Painkillers for joints. Sleeping pills for insomnia. CBT for anxiety. It was only when I started reading about perimenopause myself that I realized: one cause. Multiple symptoms. Hormones."
"Once I Started HRT, the Pain Disappeared Within Weeks"
"This is the part I wish every woman knew. I started HRT at 48 — primarily for hot flashes and insomnia. Within THREE WEEKS, my joint pain was almost completely gone. The morning stiffness that had been my daily reality for two years — gone. The knee pain climbing stairs — gone. The aching hips that woke me at night — gone. I didn't start HRT for my joints. But my joints were the first thing to respond. That told me everything I needed to know about what was causing the pain. It was hormonal. And replacing the hormones fixed it."
Why Estrogen Loss Causes Joint Pain — The Science Explained Simply
Estrogen Is an Anti-Inflammatory — And You're Losing It
This is the foundational mechanism:
Estrogen is one of the most powerful natural anti-inflammatory agents in the human body.
It suppresses pro-inflammatory cytokines (IL-1, IL-6, TNF-α) — the chemical messengers that drive pain, swelling, and tissue damage in your joints. When estrogen levels are stable and adequate, your joints exist in a relatively protected anti-inflammatory environment.
During perimenopause, as estrogen fluctuates and trends downward:
Inflammatory cytokines increase → joint tissues become more inflamed
The inflammation is subclinical — meaning it doesn't show up on standard blood tests (CRP, ESR) because it's localized, not systemic
But your joints feel it — as stiffness, soreness, aching, and reduced mobility.
This is why your blood tests can come back "normal" while your joints hurt. The inflammation is real but local — happening in the joint tissue itself, below the detection threshold of standard inflammatory markers.
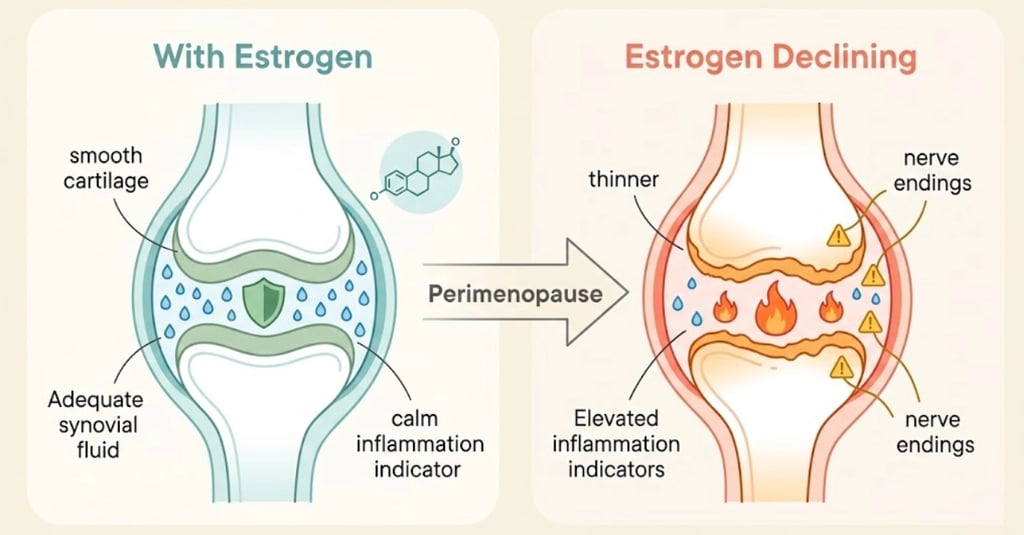
How Estrogen Protects Cartilage and Synovial Fluid
Estrogen doesn't just reduce inflammation — it actively maintains the structural health of your joints:
Cartilage:
Estrogen receptors (ERα and ERβ) are present in articular chondrocytes — the cells that maintain cartilage
Estrogen promotes chondrocyte survival and cartilage matrix production
When estrogen declines, cartilage maintenance slows → the cushioning between your bones becomes less effective → pain and stiffness increase
Synovial fluid:
Estrogen supports the production of synovial fluid — the viscous lubricant inside your joints
Adequate synovial fluid allows smooth, painless joint movement
Reduced estrogen → less synovial fluid → joints feel dry, stiff, and creaky.
Think of it this way: estrogen keeps your joints lubricated, cushioned, and calm. Remove estrogen — or make it fluctuate wildly — and your joints lose all three.
The Collagen Connection — It's Not Just Your Skin
Estrogen supports collagen production throughout the body — including in joint cartilage, tendons, and ligaments.
Research shows that women lose approximately 30% of their collagen in the first five years of menopause. This collagen loss begins during perimenopause and affects:
Joint cartilage → less cushioning
Tendons → less elasticity, more stiffness
Ligaments → less flexibility, more susceptibility to strain
Intervertebral discs → less hydration, contributing to back pain
Skin → wrinkles and loss of elasticity (the visible sign of the same process).
When women say their joints "feel old" during perimenopause, this is the biological reality: their connective tissues are experiencing collagen depletion — a process driven by hormonal change, not chronological aging.
Inflammation, Cytokines, and the Pain Cascade
Here's the cascade that produces the pain you feel:
Estrogen drops → anti-inflammatory protection decreases
Pro-inflammatory cytokines rise (IL-1, IL-6, TNF-α)
Local inflammation develops in joint synovium (lining)
Nerve endings in joint tissue become sensitized → pain threshold drops
Stiffness develops as inflamed tissue becomes less supple
Cartilage degradation may begin — potentially accelerating pre-existing wear
Pain becomes self-reinforcing — inflammation → reduced movement → more stiffness → more pain.
This cascade explains why perimenopausal joint pain often gets progressively worse over months or years if left unaddressed — and why intervening at any point in the cascade (reducing inflammation, supporting cartilage, replacing estrogen) can break the cycle.
The Estrogen-Pain Perception Link — Your Brain Feels More
There's one more mechanism worth understanding:
Estrogen modulates pain perception in the brain. It influences opioid receptors, serotonin, and norepinephrine pathways that regulate how your central nervous system processes pain signals.
When estrogen fluctuates or declines:
Pain sensitivity increases — the same stimulus produces a stronger pain signal
Pain inhibition weakens — your brain's natural "pain dampening" systems become less effective
You literally feel more pain from the same degree of joint inflammation than you would have at stable estrogen levels.
This is not "it's all in your head." This is neuroscience — your brain's pain processing system is hormonally modulated, and perimenopause changes the settings.
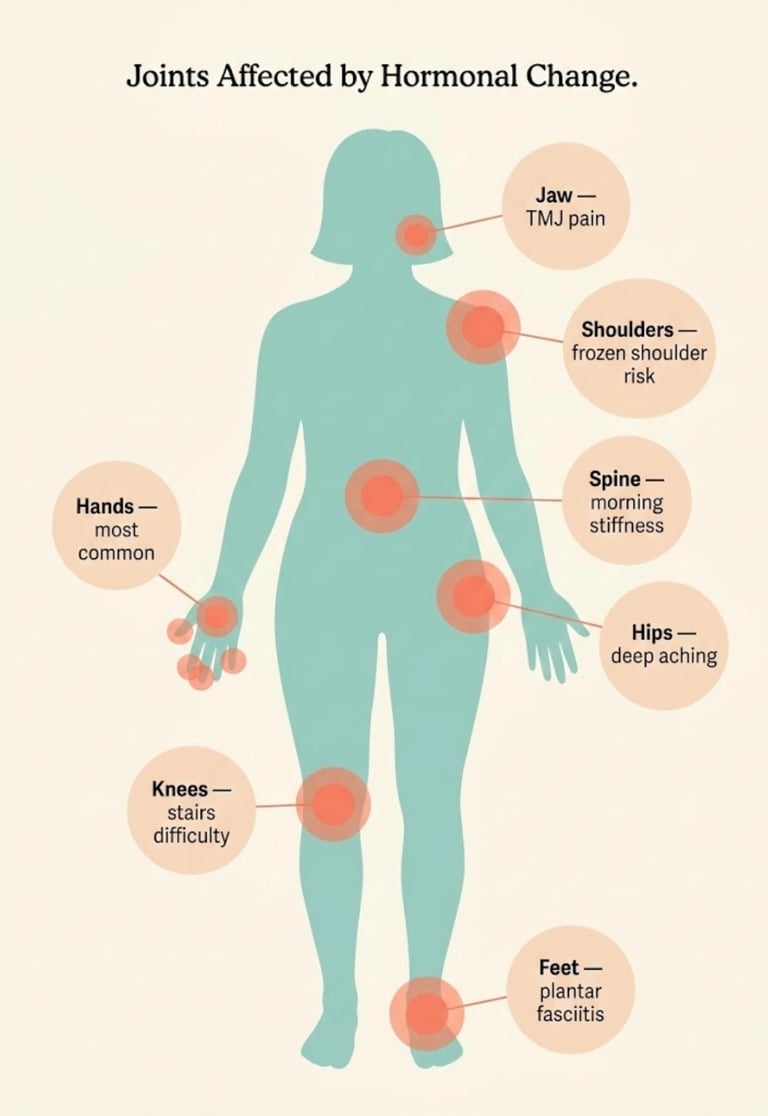
Which Joints Are Most Affected — And Why
Perimenopausal joint pain can affect any joint, but certain areas are disproportionately impacted:
Hands and Fingers
Most commonly reported. Women describe:
Morning stiffness in fingers — difficulty making a fist
Aching in the small joints of the hands (PIP and DIP joints)
Difficulty opening jars, gripping objects, typing
Rings feeling tighter (due to subtle inflammatory swelling)
Sometimes trigger finger — a catching or locking sensation when bending a finger.
Why hands are vulnerable: Hands have the highest density of small joints in the body, each with estrogen-responsive synovial tissue. The cumulative effect of estrogen decline across many small joints is amplified here.
Diagnostic caution: Hand joint pain in women over 40 is very frequently attributed to osteoarthritis (OA) — and sometimes it IS OA. But in many cases, the hormonal component is either the primary cause or a significant contributor. If your hand pain appeared coincident with perimenopausal symptoms, hormones should be considered.
Knees
Aching when climbing or descending stairs
Stiffness after sitting for extended periods (the "movie theater effect")
Pain during or after squatting or kneeling
A sense that your knees are less stable or less trustworthy.
Why knees are vulnerable: Knee joints bear significant load and are particularly dependent on cartilage health and synovial lubrication — both of which decline with estrogen loss. The menisci (cartilage cushions in the knee) have estrogen receptors and are directly affected.
Hips
Deep aching in the hip joint — sometimes felt in the groin or outer hip
Morning stiffness that requires several minutes of walking to ease
Pain at night — especially when lying on the affected side
Reduced range of motion — feeling like your hips are "tight" or restricted.
Why hips are vulnerable: The hip is a large ball-and-socket joint with substantial cartilage and synovial membrane — all estrogen-responsive. Trochanteric bursitis (inflammation of the bursa on the outer hip) is also more common during perimenopause.
Shoulders and Frozen Shoulder
General shoulder aching and stiffness
Reduced range of motion — difficulty reaching behind your back or overhead
Frozen shoulder (adhesive capsulitis) — a specific condition where the shoulder capsule becomes inflamed and progressively stiff.
The frozen shoulder connection:
This deserves special attention. Adhesive capsulitis peaks in women aged 40–60 — and emerging research strongly suggests a hormonal link:
Women are affected more often than men
The peak incidence coincides with perimenopause and early postmenopause
Estrogen receptors have been identified in shoulder capsule tissue
Some clinicians report that frozen shoulder responds to HRT — though controlled trials are limited
A 2019 study in BMJ Open found that women undergoing menopausal transition had significantly higher rates of frozen shoulder.
If you've developed frozen shoulder in your mid-40s to early 50s without a clear injury, hormones may be a contributing factor.
Spine and Lower Back
New or worsening lower back stiffness
Difficulty with prolonged sitting or standing
Pain that's worse in the morning and improves with movement
Sometimes associated with disc dehydration — estrogen supports the water content of intervertebral discs.
Feet, Ankles, and Plantar Fasciitis
Heel pain (particularly first steps in the morning) — classic plantar fasciitis
Aching in the small joints of the feet (metatarsals)
Ankle stiffness
Reduced tolerance for standing or walking.
The perimenopause-plantar fasciitis connection: Plantar fasciitis involves inflammation and degeneration of the plantar fascia — a thick band of collagen-rich connective tissue. Estrogen decline reduces collagen quality and increases inflammatory tendency in this tissue. Women in their 40s and 50s are disproportionately affected.
TMJ and Jaw Pain
Jaw stiffness or aching — especially on waking
Clicking or popping of the jaw joint
Difficulty opening the mouth fully
Headaches originating from jaw tension.
Why TMJ is hormonal: The temporomandibular joint has estrogen receptors, and estrogen influences the inflammatory and pain-modulating environment of the joint. TMJ symptoms are more common in women, and fluctuations in estrogen may contribute to onset or worsening during perimenopause. Increased jaw clenching due to perimenopausal anxiety and sleep disruption also contributes.
Is It Perimenopause — Or Something Else?
This is the critical question — and the one that causes the most confusion and the most unnecessary worry.
The good news: In most cases, joint pain that appears in a woman between 40 and 55, alongside other perimenopausal symptoms, and with negative autoimmune markers, is hormonal.
The responsible message: But hormonal joint pain can coexist with other conditions — and some conditions do need to be identified and treated specifically. Here's how to differentiate:
Perimenopause Joint Pain vs. Rheumatoid Arthritis (RA)
Key distinction: If morning stiffness lasts more than 60 minutes consistently, visible joint swelling is present, or symptoms are worsening rapidly, rheumatoid arthritis should be excluded before attributing pain to hormones alone.
Perimenopause Joint Pain vs. Osteoarthritis (OA)
Important nuance: Perimenopause can accelerate pre-existing osteoarthritis. If you already had mild OA, the loss of estrogen's anti-inflammatory and cartilage-protective effects may make it worse. In these cases, both hormonal and structural factors contribute — and both should be addressed.
Perimenopause Joint Pain vs. Fibromyalgia
Overlap alert: Fibromyalgia onset peaks in women during perimenopause and early postmenopause. The conditions can coexist, and hormonal changes may trigger or worsen fibromyalgia in susceptible women.
Perimenopause Joint Pain vs. Thyroid-Related Joint Issues
Hypothyroidism can cause joint stiffness, muscle aches, and pain — symptoms that closely mimic perimenopausal joint pain.
Thyroid dysfunction becomes more common in women over 40
It can coexist with perimenopause
A thyroid panel (TSH, Free T4, Free T3, thyroid antibodies) should be part of the evaluation for any woman with new joint pain during midlife.
Key distinguisher: Hypothyroidism typically also causes cold intolerance, constipation, dry skin, and weight gain with a sluggish quality — whereas perimenopause more often causes hot flashes, irregular periods, and temperature dysregulation upward.
When Both Exist — Hormones and Pre-Existing Conditions
Here's the reality that nuanced care requires:
Hormonal joint pain can exist ALONGSIDE other conditions. A woman can have:
Mild osteoarthritis plus hormonal joint inflammation
Early rheumatoid arthritis triggered or worsened by hormonal shifts
Fibromyalgia emerging during the menopausal transition
Hypothyroidism compounding perimenopausal symptoms
The best approach isn't to pick one diagnosis — it's to consider all contributing factors and address them in parallel.
The Tests Worth Requesting
If you're experiencing new or worsening joint pain during your 40s or 50s, these investigations help rule out other causes and build the case for hormonal management:
The likely result in hormonal joint pain: RF negative. Anti-CCP negative. CRP normal or mildly elevated. ESR normal. ANA negative. X-rays unremarkable or showing age-appropriate minor changes. Vitamin D possibly low. Thyroid possibly borderline.
What this tells you: Your joints are structurally sound. The pain is driven by the hormonal-inflammatory environment — which is exactly what estrogen decline creates.
What Science Says — The Evidence Behind Hormonal Joint Pain
Estrogen Receptors in Joint Tissue — The Research
The connection between estrogen and joints isn't speculative — it's grounded in receptor biology:
Estrogen receptors (ERα and ERβ) have been identified in articular cartilage, synovial tissue, ligaments, tendons, and bone (research published in Arthritis & Rheumatism)
Estrogen directly influences chondrocyte metabolism — the cells that maintain cartilage health
Estrogen modulates matrix metalloproteinases (MMPs) — enzymes that break down cartilage. Less estrogen → more MMP activity → more cartilage degradation
Synovial fibroblasts (cells lining the joint) respond to estrogen by regulating inflammation and fluid production
This is not a hypothetical connection. It's documented cellular biology.
The Menopause-Osteoarthritis Acceleration
One of the most consistent findings in orthopedic research:
The incidence of osteoarthritis increases dramatically in women after menopause — far exceeding the increase seen in age-matched men.
Before menopause, OA rates are similar between sexes. After menopause, women's rates surge past men's — particularly in the hands and knees. This strongly implicates estrogen loss as a causal or accelerating factor in osteoarthritis development.
Research from the Women's Health Initiative (WHI) found that women on HRT had lower rates of joint replacement surgery compared to non-users — suggesting a protective effect of estrogen on joint health.
What's Established vs. What's Still Being Studied
Scientifically established:
Estrogen receptors exist in all major joint tissues (cartilage, synovium, ligaments, tendons)
Estrogen has anti-inflammatory and cartilage-protective properties
Musculoskeletal symptoms affect 50–60% of women during the menopausal transition
Osteoarthritis incidence increases sharply after menopause
Many women report significant improvement in joint symptoms with HRT
Probable (growing evidence):
Frozen shoulder has a significant hormonal component
Tendinopathies (plantar fasciitis, carpal tunnel, trigger finger) may be partly estrogen-mediated
Early HRT initiation may offer long-term joint and cartilage protection
Collagen supplementation may support estrogen-depleted connective tissue
Still debated or under-researched:
Whether HRT can reverse (not just prevent) cartilage damage
Optimal timing and duration of HRT for joint-specific benefits
The relative contribution of hormonal vs. mechanical factors in perimenopausal OA
Whether testosterone also plays a role in joint health in women
This article is for educational purposes and does not replace medical advice. Joint pain during perimenopause is common and usually benign, but new or worsening joint symptoms should be evaluated by a healthcare provider to rule out other conditions.
What Actually Helps — Evidence-Based and Real-World Solutions
Hormone Therapy — The Most Direct Approach
For women whose joint pain is primarily hormonal, HRT is often the most effective treatment — sometimes dramatically so.
What the evidence shows:
Multiple observational studies report significant improvement in joint pain and stiffness with HRT
The WHI data showed lower rates of joint arthroplasty in HRT users
Many menopause specialists report that joint pain is one of the most responsive symptoms to HRT — sometimes improving within 2–4 weeks
Both systemic estrogen and combined HRT (estrogen + progesterone) can help
How it works:
Estrogen replacement restores the anti-inflammatory environment in joint tissues
It supports synovial fluid production and cartilage maintenance
It normalizes pain processing in the central nervous system
The result: less inflammation, better lubrication, less pain sensitivity
What to discuss with your provider:
Whether you're a candidate for HRT (based on your health history and risk factors)
Which formulation is appropriate (transdermal estrogen is often preferred for its safety profile)
How to monitor response — joint pain should begin improving within 4–8 weeks if hormones are the primary driver
Important: If your joint pain doesn't improve with HRT, that's valuable diagnostic information — it suggests other factors (structural, autoimmune, nutritional) are contributing and should be investigated further.
Anti-Inflammatory Nutrition
Diet can't replace hormones — but it can meaningfully reduce the inflammatory load on your joints:
Foods that support joint health:
Foods that tend to worsen joint pain:
The pattern: A Mediterranean-style, anti-inflammatory dietary approach — high in omega-3s, vegetables, olive oil, and lean protein, low in processed foods and sugar — is consistently associated with lower inflammatory markers and better joint outcomes in midlife women.
Movement and Exercise — The Right Types Matter
Exercise is essential for joint health during perimenopause — but the type matters:
Best types for perimenopausal joints:
Types to modify or approach carefully:
High-impact activities (running, jumping, HIIT) — may aggravate inflamed joints. Not necessarily off-limits, but listen to your body and modify if pain increases
Excessive static stretching — overstretching estrogen-depleted ligaments may increase injury risk
Complete inactivity — the WORST thing for perimenopausal joints. Immobility → less synovial fluid → more stiffness → more pain
The exercise paradox: Movement often hurts initially but reduces pain long-term. Gentle, consistent movement is the most effective non-medical treatment for hormonal joint pain. Start slowly, increase gradually, and prioritize consistency over intensity.
Supplements With Evidence (And Those Without)
What NOT to waste money on:
Any supplement claiming to "cure" arthritis or "rebuild" joints — exaggerated claims signal low-quality products
High-dose single vitamins without testing for deficiency first
Unregulated proprietary blends without transparent ingredient lists
Pain Management Strategies
For days when the pain is significant:
Ibuprofen or naproxen (NSAIDs) — effective anti-inflammatories. Use as needed, not as a daily long-term strategy (discuss with your doctor if using regularly)
Topical anti-inflammatories (diclofenac gel/Voltarol) — applied directly to painful joints. Lower systemic absorption than oral NSAIDs
Heat therapy — warm baths, heat packs, heated blankets. Heat increases blood flow and synovial fluid production
Cold therapy — ice packs for acute pain or after exercise-triggered inflammation (15–20 minutes maximum)
Epsom salt baths — magnesium sulfate absorbed through skin may support muscle relaxation. At minimum, the warm bath helps
Gentle morning stretching routine — a 5–10 minute stretch sequence before getting out of bed can significantly reduce morning stiffness
Compression gloves (for hand pain) — some women find these helpful for nighttime hand stiffness
Body Work and Physical Therapy
Physiotherapy/Physical therapy — a physiotherapist can design a joint-specific exercise program and address biomechanical issues
Massage therapy — reduces muscle tension around painful joints and improves local circulation
Acupuncture — some women report benefit for joint pain. Evidence is modest but positive for osteoarthritis-related pain
Pelvic floor physiotherapy — if hip or lower back pain is involved, pelvic floor dysfunction (common in perimenopause) may be contributing

🔎 Recommended Tools and Resources
This article may contain affiliate links. We only recommend products we've researched and believe may be genuinely useful for women navigating perimenopause. Affiliate commissions help support this site at no extra cost to you.
1. Omega-3 Fish Oil (High-Potency EPA/DHA)
Best for: Systemic anti-inflammatory support — joints, heart, brain, skin
Why it helps here: EPA and DHA omega-3s are the most evidence-backed dietary anti-inflammatory compounds. They directly reduce the pro-inflammatory cytokines (IL-6, TNF-α) that drive perimenopausal joint pain
Evidence level: Strong for anti-inflammatory benefit. Moderate for joint pain specifically
What to look for: Minimum 1,000 mg combined EPA+DHA per serving. Triglyceride form. IFOS-certified for purity. Third-party tested
Timeline: 4–8 weeks for noticeable benefit
Limitations: May interact with blood-thinning medications. Quality varies enormously across brands
2. Vitamin D3 + K2 Supplement
Best for: Bone and joint support — especially if deficient (and most women in northern climates are)
Why it helps here: Vitamin D deficiency contributes to bone pain, muscle weakness, and joint discomfort. K2 directs calcium to bones and away from soft tissues. Together, they support the skeletal system that perimenopause is stressing
Evidence level: Strong for correcting deficiency. Supplementation without deficiency testing is less clear
Important: Test your vitamin D level before supplementing. Target: 50–80 nmol/L (UK) / 40–60 ng/mL (US)
Limitations: Fat-soluble — take with a meal containing fat. Excess vitamin D can be harmful; don't mega-dose
3. Collagen Peptides (Type I & II)
Best for: Supporting cartilage, tendon, and connective tissue health during collagen decline
Why it helps here: Perimenopause accelerates collagen loss. Hydrolyzed collagen peptides provide the amino acids (glycine, proline, hydroxyproline) that are building blocks for cartilage and connective tissue. Emerging research suggests supplementation may support joint comfort
Evidence level: Emerging — several positive studies but not yet definitive. Biologically plausible
Dosage: 10–15 grams daily, dissolved in liquid
Limitations: Results take 8–12 weeks. Not all collagen supplements are equal — look for hydrolyzed peptides from reputable sources. Bovine or marine sourced
4. "The New Menopause" by Dr. Mary Claire Haver
Best for: Comprehensive understanding of how perimenopause affects the body — including musculoskeletal health — and what treatment options exist
Why it helps here: Covers the inflammatory mechanisms driving perimenopausal symptoms, including joint pain. Discusses HRT, anti-inflammatory nutrition, and the Galveston Diet approach — all relevant to managing hormonal joint pain
Strengths: Action-oriented, evidence-based, covers nutrition and medical options together
5. Heated Hand/Joint Wrap (Reusable)
Best for: Immediate morning stiffness relief — especially for hands, wrists, and knees
Why it helps here: Heat increases blood flow and synovial fluid production in joints. A microwavable joint wrap applied for 10–15 minutes in the morning can significantly reduce the "cold start" stiffness that perimenopausal women experience
Practical benefit: Simple, drug-free, and effective for daily management. Can be used alongside any other treatment
Limitations: Symptomatic relief only — doesn't address root cause. Avoid on acutely inflamed or swollen joints (use cold instead)
YMYL disclosure: No supplement replaces medical evaluation or hormone therapy for significant perimenopausal joint pain. These products may offer supportive benefit alongside professional care. Vitamin D and omega-3 have the strongest evidence base; collagen is emerging. Always consult your healthcare provider before starting new supplements, especially with existing conditions or medications.
How to Talk to Your Doctor About Hormonal Joint Pain
What to Say — And What to Ask For
The language you use can make the difference between a productive appointment and a dismissive one.
Opening statement:
"I've developed new joint pain over the past [X months]. I'm also experiencing [list other perimenopause symptoms: irregular periods, insomnia, hot flashes, mood changes]. I believe the joint pain may be connected to perimenopause. I'd like to discuss this possibility and explore appropriate investigations and treatment options."
Specific questions to ask:
"Can we run blood tests to rule out rheumatoid arthritis and thyroid issues?" (RF, anti-CCP, CRP, ESR, TSH, Free T4)
"Can we check my vitamin D level?" (Deficiency is common and easily correctable)
"Could hormone therapy help my joint symptoms, given my other perimenopausal symptoms?"
"Would you consider referring me to a menopause specialist if hormonal treatment is outside your expertise?"
"Can we also check my ferritin? I want to rule out iron deficiency contributing to my fatigue and pain."
When to Push for a Referral
Consider pushing for a referral if:
Your GP dismisses joint pain as "just aging" without investigation
You've had negative autoimmune tests but no one has discussed hormonal causes
You want to explore HRT specifically for joint symptoms and your GP is unfamiliar or uncomfortable with this
Your joint pain is significantly impacting your quality of life and first-line treatments aren't helping
Where to seek help:
NAMS-certified menopause practitioner — understands the hormonal contribution to joint pain
Rheumatologist — to rule out autoimmune and inflammatory conditions (essential if there's diagnostic uncertainty)
Physiotherapist — for exercise-based management and biomechanical assessment
Integrative medicine physician — may offer a more holistic approach combining hormonal, nutritional, and lifestyle strategies
Building Your Case With Data
Track the following for 4–8 weeks before your appointment:
Which joints hurt — and when
Severity (1–10 scale, daily)
Morning stiffness duration (minutes)
Menstrual cycle correlation — is pain worse at certain cycle points?
Sleep quality — poor sleep often amplifies pain
Other perimenopause symptoms — documenting the full picture strengthens the hormonal case
What helps and what worsens the pain
This data transforms "my joints hurt" into "I have a documented pattern of multi-joint pain that correlates with my perimenopausal symptoms, worsens premenstrually, and is not explained by autoimmune testing."
That's a much harder case to dismiss.
Your Joints Aren't Aging Overnight — They're Adapting to a Hormonal Shift
If you've been living with perimenopausal joint pain — whether for weeks or years — here's what we want you to take away:
Your pain is real. It has a biological explanation grounded in receptor biology, inflammatory pathways, and collagen metabolism. It's not "in your head." It's not "just aging." And it's not your fault.
Your pain is explainable. Estrogen has been protecting your joints — lubricating, cushioning, calming inflammation, and maintaining cartilage — for your entire adult life. When estrogen fluctuates and declines, your joints feel the loss. Every ache is a signal, not a mystery.
Your pain is treatable. HRT, anti-inflammatory nutrition, movement, supplements, and pain management strategies can — individually or in combination — make a meaningful difference. Many women report dramatic improvement. You don't have to accept this as your new normal.
Your pain is temporary — in its current form. For most women, the acute hormonal joint pain of perimenopause stabilizes or improves as hormones settle after menopause — especially with appropriate support. The most intense phase is often the transition itself.
You deserve a doctor who connects the dots. If your provider hasn't considered hormones as a cause of your joint pain, you now have the language, the science, and the framework to start that conversation. You're not being a difficult patient. You're being an informed one.
Your joints aren't failing. Your body isn't falling apart. Your hormones are shifting — and your joints are telling you about it. Listen. Investigate. Seek support. And know that on the other side of this transition, your body can feel good again.
FAQ — Perimenopause Joint Pain
Q: Can perimenopause cause joint pain?
A: Yes. Estrogen has anti-inflammatory properties and supports cartilage, synovial fluid, and collagen in joint tissues. When estrogen fluctuates during perimenopause, joints lose this protection — resulting in stiffness, aching, and pain. An estimated 50–60% of women experience musculoskeletal symptoms during the transition.
Q: What does hormonal joint pain feel like?
A: Hormonal joint pain typically involves morning stiffness lasting 10–30 minutes, a deep aching in multiple joints (especially hands, knees, and hips), pain that moves between joints, and symptoms that fluctuate with your menstrual cycle. It often feels like "overnight aging."
Q: Does HRT help with perimenopause joint pain?
A: For many women, yes — sometimes dramatically. HRT restores the anti-inflammatory environment in joints, supports synovial fluid production, and reduces pain sensitivity. Some women report significant improvement within 2–4 weeks of starting hormone therapy.
Q: How do I know if my joint pain is perimenopause or arthritis?
A: Hormonal joint pain typically produces negative autoimmune markers (RF, anti-CCP), minimal visible swelling, morning stiffness under 30 minutes, and appears alongside other perimenopause symptoms. Rheumatoid arthritis usually shows positive blood markers, visible swelling, and stiffness lasting over 60 minutes. Both can coexist.
Q: Which joints are most affected by perimenopause?
A: Hands and fingers are most commonly affected, followed by knees, hips, shoulders, lower back, and feet. Frozen shoulder and plantar fasciitis also peak during perimenopause and may have hormonal components.
Q: Can supplements help perimenopause joint pain?
A: Omega-3 fish oil has moderate-to-strong evidence for reducing inflammation. Vitamin D is essential if deficient. Collagen peptides show emerging promise. Curcumin may help. These work best as supportive measures alongside medical treatment and lifestyle changes — not as standalone solutions.
Ready to take the next step?
(https://perimenopausecompass.com/free-14-day-tracker) to find your personal triggers.
Get the Perimenopause Nutrition Protocol to support your nervous system from the inside out.
Visit our (https://perimenopausecompass.com/start-here) page for more foundational guidance.
Get the Perimenopause Nutrition Protocol ($29 + bonus) → https://perimenopausecompass.gumroad.com/l/iecoc
______________________________________
Disclaimer Education only — not medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Sources / References
Perimenopause Compass
Contact
hello@perimenopausecompass.com
© 2026 All rights reserved.